
In September 2013, Liz – a 54-year-old Indonesian – has pains around her right rib-cage. An USG indicated fluid in her lungs. Liz was referred to a lung specialist who thought she had tuberculosis (TB). Liz was prescribed TB medication for three months.
After three months, there was again fluid in her lungs. About 1.3 litres of fluid was tapped out. Liz was told to continue taking her TB medication.
Liz went to Jakarta and consulted another doctor. Pleural tapping was again done and 0.6 litre of fluid was removed from her lung. Liz was again asked to continue with her TB medication.
Not satisfied Liz went to Singapore. Blood test, CT and PET scan were performed (note: no CT or PET scan were ordered by doctors in Indonesia).
Blood test results, 14 April 2014
| Alkaline phosphatase | 188 (H) |
| AST/SGOT | 84 (H) |
| ALT/ SGPT | 83 (H) |
| GGT | 100 (H) |
| CEA | 44.3 (H) |
| CA 125 | 26.6 (H) |
| CA 19.9 | 4.6 |
| AFP | 6.4 |
CT Scan of the Thorax, 14 April 2014
- A large right -side pleural effusion is seen involving the upper lobe of the right lung and extending to involve the middle lobe.
- Suspicious of a nodular mass more than 2 cm in size present in the upper lobe of the right lung.
- Presence of a small nodule in the left lung in the lower lobe, 6 mm in size. This is suspicious of a possible metastatic lesion.
Cytopatholoogy report of right pleural fluid, 14 April 2014
- pleural fluid negative for maligancy.
- pleural fluid is haemorrhagic with few inflammatory cells and an occasional mesothelial cell.
PET/CT Study on 15 April 2014
- Hypermetabolic mass in the upper lobe of the right lung is consistent with pulmonary malignancy.
- Mildly hypermetabolic paratracheal and precarinal nodes are suspicious of nodal metastasis. Multiple nodules scattered in both lungs are suspicious of pulmonary metastasis.
- Hypermetabolic lytic lesions in the thoracic vertebra and left ischium are compatible with metastases.
Cytopathology report – FN lung biopsy, 17 April 2014
Malignant cells present consistent with infiltrative moderately differentiated pulmonary adenocarcinoma.
MRI Brain
No MRI imaging evidence of intracranial metastatic disease is detected.
Liz was not able to walk by herself and had to use the wheel chair. She received 10 sessions of radiation treatment. After radiotherapy, she was able to walk. But she still had cramps and numbness in her legs. Liz told us that this leg numbness and cramp developed after 2 months on the TB medication.
For her lung cancer, the oncologist prescribed Iressa, costing SGD 3,500 per month.
Meaningless temporary decrease of CEA after taking Iressa
| April 2014 | Started on Iressa, CEA = 44.3 |
| 11 June 2014 | X-ray chest: Slight interval improvement. CEA = 18.7 (decrease from 44.3) |
| 13 August 2014 | X-ray chest: Stable lobulated opacity seen. CEA = 31.2 (started to increase) |
| 14 October 2014 | X-ray chest: No significant change. CEA = 36.0 (slight increase) |
| 20 January 2015 | X-ray chest: Right pleural effusion is stable. CEA = 47.6 (increase from initial value) |
Meaningless improvements of PET scan images after taking Iressa (Study of April 2014 versus October 2014).

(Top: April 2014 after Iressa bottom: October 2014)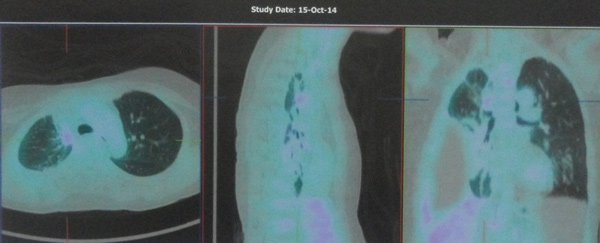
(Left: April 2014 after Iressa right: October 2014)
Iressa did not help Liz. The oncologist offered two options:
- Stop taking Iressa and go for chemothrapy.
- Or continue taking Iressa for another 2 months and see what happen.
Liz decided to stop further medical treatment and came to seek our help.

You must be logged in to post a comment.