CK is a 62-year-old male from Kuala Lumpur. He and his wife came to see us with copies of his medical reports neatly filed in a folder. This is a very pleasant couple who is now helpless and directionless. This is what happened.
1) 20 December 2015: Had food poisoning after taking expired red wine.
2) 21 December 2015: Consulted a GP who discovered “cracking sound” in his left lung.
3) 22 December 2015: CT scan of chest showed a 3.2 x 5 cm mass in the left lung.
4) 2 January 2016: A CT-guided biopsy confirmed a bronchoalveolar adenocarcinoma.
CK was referred to a cardio-thoracic surgeon in a “heart hospital.”
5) 14 January 2016: PET scan confirmed carcinoma of the left lung with no associated locoregional or distant metastasis.
6) 23 January 2016: Admitted to the “heart hospital” for lower lobe lobectomy, i.e. surgery to remove a quarter of the lung.
The surgery was a “success” and histopathology report showed:
a) Aortic wall adventitia was infiltrated by tumour.
b) One pulmonary lymph node showed tumour metastasis.
c) lower lobe of left lung — invasive adenocarcinoma with predominant bronchoalveolar and papillary pattern.
7) February to June 2016: Underwent 4 cycles of chemotherapy and 20 sessions of radiotherapy.
Things seemed to be okay after all these treatments but CK had chest pains, coughs and fever. He was prescribed “strong” antibiotics.
8) 30 March 2017 — after slightly more than a year.
Follow up CT scan showed multiple nodules and patchy opacities in the upper and lower lobes of right lung.
Radiologist suggested: Differential diagnosis: lung metastases and pneumonia. Suggest close follow up CT lung after a course of antibiotics.
CK went back to his surgeon about this new development. The surgeon was pretty sure that the spots were not cancer related.
9) 1 June 2016: CT scan of chest. The radiologists wrote the following:
CT on 23 March and 30 March 2017 were reviewed. The current CT is about 2-3 months after the previous CTs. The current CT showed the following:
a) The ground glass opacities in the right upper and lower lobes of the lung appears more dense and larger.
b) Newer small nodular lesions are seen in the right upper and lower lobes.
Based on the above observations, the radiologist was of the opinion that this new development was a metastasis or recurrence. However, ground glass opacities may be due to drug induced lung changes and infection.
The changes in the left upper lobe (note: left lower lobe was removed) are suggestive of non-neoplastic process and fibrosis. If DXT (radiotherapy) was given, these could be due to that treatment.
10) 18 September 2017: Went back to the same GP again (as in 2). “Cracking sound” at the lower part of my good lung.
Cancer marker in December 2016 was 16. In July 2017,it was 173.
CK and his wife decided not to go back to his doctors again. Because it will just be repeating the same procedures all over again — another biopsy and more chemo.
Total cost of treatment = RM130,000 of personal savings.
Comments
I had my first lesson about lung cancer some 22 years ago. The second patient of CA Care is VJ. He had lung cancer and had one side of his lung removed and underwent treatments at the “cancer hospital.” I was at the hospital and saw him suffer and eventually died.. Surgery did not cure lung cancer. Treatments received in the cancer hospital also did not cure lung cancer.
My second lesson about lung cancer came a few years later when the mother of my student underwent radiotherapy for her lung cancer. Yes, I encouraged her to go for the treatment. After completion of her treatment she died. Lesson number two, radiation does not cure lung cancer. To understand why, just go to the market and buy a piece of lung. Bring home and place the lung over fire and see what happen! The lung hardened — and is this not why the patient cannot breath?
Over the years, I have seen this story being repeated over and over again. In the case of CK, it is another one of those cases I have come across over the years.
Can herbs cure CK’s cancer? No. Can we help him? May be. CK’s problem recurred less than 2 years after treatment. After spending RM 130,000 he got nothing out of it.
Perhaps some people would want to tell you that if you don’t go for treatment, you would die sooner. Nope — I don’t believe so. Over the years, I have patients who led a much better life if they do nothing.
Perhaps you may want to read some of the articles I have written earlier:
Don’t give up hope yet. We shall do our best. If you can sleep, can eat, can move around and have you no pain, don’t ask for more. To that CK and his wife totally agreed. In fact that was what they hope for when they came to seek our help … “to have quality life.”
We felt sorry for SF, her hope crushed. After 12 cycles of chemo and spending RM 150,000, she was told the tumors had shrunk and she was cured! (Or did she misunderstood her doctor’s message?). But after one month at home, she had bleeding and came back to her doctor again. Her tumour had grown back to its original size. It was a failure. Her doctor did not have time for her and hurriedly told her to for surgery.
With wounded feelings she and her husband left the hospital and sought the help of another oncologist in another hospital. She was started on radiotherapy to be followed by chemotherapy. We felt SF should just continue with her medical treatment and not take our herbs yet. We sent set her away without any herbs.
SF and her husband came back to see us again after a few days. We spent almost 2 hours talking. It was a “heart-breaking” morning for me. I laid out my advice as clearly, honestly and bluntly as possible. But I was mindful not to cause panic or to instill fear in her. Many times during our conversation, I asked her and her husband to think clearly and deeply the implications of what she wanted to do. She should then make her own decision based on what her heart wanted, after considering various points I raised.
What did you get out of your failed RM150,000 treatment?
Diarrhea after radiotherapy
Patient: I had diarrhea after the radiation.
C: Did you have any diarrhea before you went for radiation?
P: No, the diarrhoea started 2 days after the radiation (note: it continued as of this writing — already 3 weeks).
C: I really cannot tell you what else can happen after this. Did you ever ask the doctor if these treatments — radiation and chemotherapy — are going to cure you?
P: No, we never ask.
C: You should ask before you undergo all these!
Tumor shrunk after the first round of chemotherapy!
P: After 6 cycles of chemo, I was told the tumour had shrunk. And I needed another 6 more cycles. The doctor said I was cured. I requested the doctor to do a CT scan for me to confirm the result. The doctor said, No need, you are already cured. Go home.
C: What? He said chemo cured you?
P: He asked me to come back after 2 months for review. But one month at home, I had bleeding and we brought forward our travel and came back to see the doctor again.
Husband: The tumour had grown bigger (back to its original size, see table below).
C: Did you ask the doctor why? Only last month he said you were already cured. Now, what happened.
P The doctor was angry.
C: Har?
H: We were confused. We returned to see the doctor one day before he was to go on leave. It seemed he was “uncomfortable” and told us crudely — You just go for the operation! We then went to see another oncoloogist in another hospital.
Elevated liver function parameters
C: Let’s look at your liver function results (table below).
On 8 June 2016, after finishing 6 cycles of chemo, your liver function was still okay. But you see what happened after you did 12 cycles of chemo. All the liver enzymes values were elevated. Your liver was going downhill. Okay, some people may want to rationalize that it is normal after chemotherapy. The liver function enzymes will go back to normal again after you stop chemo. Well, I don’t know if you want to believe that or not.
You are going to be given more chemo. I cannot tell you what is going to happen to your liver after this. I don’t know how many more cycles of chemo they are going to give you, and what drugs they want to use. If they give you the more toxic or aggressive drugs, what is going to happen to your liver?
They want to give you more chemo because they hope to shrink the tumour before they proceed with surgery. You have already done 12 cycles of chemo in Hospital A before. The tumour shrunk and grew back after a month. Think carefully, what do you hope to achieve this time with chemotherapy? Shrink the tumour again?
Lung nodules disappeared
P: The doctor told me that the nodules in my lungs were all gone after the chemotherapy. At least, my lungs are free of cancer.
C: Wrong Ibu (mama)! Yes, the lung nodules were completely gone after the chemo but in the October 2016 scan, there was again a 0.6cm nodule in your lung. So the impression you had was wrong.
P: I did not know this. I did not understand all this. Only now that you have told me this.
Chemotherapy means sufferings
C: Two days ago, a lady came to see me on behalf of her elderly father who had lung cancer. She consulted the same oncologist (the second oncologist, not the first oncologist in Hospital A) that you went to. This oncologist told the lady that her father needs chemo but chemo is going to cause many side effects and he would suffer. The oncologist also said that the father could go for oral drug. But oral chemo-drug can also cause sufferings.
On hearing this, the daughter “ran away” and would not want any more medical treatment for her father! At least we should be glad that this oncologist was honest to tell us this.
Patients are an ignorant lot!
C: This episode really make me sad. For years I have been trying to “educate” patients. I wonder if I have failed miserably? I understand all that you have said and gone through. You put your full trust in your doctors — they are your gods — and the gods failed you!
Also, unfortunately some of these gods are not honest. They don’t tell you the whole truth that you need to know.
P: Indeed I don’t understand all these.
C: You came to see me twice. I have explained to you what I know and I ask you to think carefully what you want to do.
H: Before this I believed that after the surgery — the tumour gone — all problems would be solved! That was what I thought. I did not know all these before your explanation. Now, I understand and realise the implications.
P: I was hoping that after the chemo, I would be cured. I did not want to go for surgery!
SF is a 56-year-old Indonesian lady. She and her husband came to talk to us, wanting to explore a way out of her dilemma.
SF’s problem started in February 2016, after she started to have bloated stomach with pain. She went to a hospital in Surabaya and was asked to undergo an operation. She decided to come to Penang to seek a second opinion.
A CT scan on 28 April 2016 indicated the following:
Multiple metastatic nodules in both lung fields measuring 0.4 to 2.5 cm.
There is an irregular complex solid and cystic mass in the retroperitoneum right lumbar region and hemipelvis. It measures 7.2 x 10.6 cm. The mass encases the right lower ureter causing severe right hydroureteronephrosis.
The left kidney is normal.
There are several enlarged para-aortic nodes noted measuring 0.6 to 1.0 cm.
Impression:
Findings suggestive of right CA ovary or retroperitoneal tumour with encasement of right lower ureter.
Subacute distal small bowel obstruction.
Multiple metastatic lesions in both lungs fields and para-aortic lymphadenopathy.
According to the doctor in Penang the tumour was too big and surgery was not indicated. SF was asked to undergo chemotherapy instead. She had 6 cycles of chemo using Gemzar and Kemocarb. The treatment cost RM 3,000 per cycle.
A CT scan done on 29 June 2016 indicated the following:
The urothelial carcinoma in the retroperitoneum right lumbar region is significantly smaller in size measuring 3.5 x 4.0 cm (previously it was 7.2 x 10.6 cm).
2.The metastatic lung nodules are completely resolved.
The oncologist considered the result a “great success”. SF was told she need NOT have to undergo any surgery. SF underwent another 6 cycles of chemo. This round the cost of each cycle was RM3,000 to RM4,000. The drugs used were the same as before.
SF was asked to go home and come back for a check-up after two months. But it was not to be, after a month at home SF had bleeding and she came back to Penang again on 4 October 2016.
A CT scan on 5 October 2016 indicated the following:
The previously noted urothelial carcinoma in the retroperitoneum at right lumbar region is significantly increased in size measuring 7.7 cm x 9.2 cm compared to the previous measurement of 3.5 x 4.0 cm.
There are multiple small subcentimeter para-oartic nodes noted, the largest measuring 12 mm in size.
In the lung bases, the previously noted small nodules seen at the left lower lobe had slightly reduced in size measuring 0.6 cm compared to the previous measurement of 0.9 cm.
A calcified uterine fibroid noted measuring 4.2 cm x 4.2 cm.
Impression:
The previously noted urothelial carcinoma in the retroperitoneum at right lumbar region is significantly increased in size with obstructive uropathy.
Unfortunately, the doctor who attended to SF was going on leave. Without much explanation, SF was just told to go and have an operation. SF consulted an urologist in the same hospital and was told the tumour was too big and surgery was not indicated. SF was asked to go for chemotherapy and radiation again.
Disappointed and not satisfied, SF went to see another oncologist in another hospital. She was told the following:
Operation would be too risk.
Not all tumour could be removed.
The surgery would possible make the cancer spread faster.
The only option left was chemo and radiation. SF agreed to this third round of treatment. She received 5 sessions of radiation. This cost RM 6,700. The chemo was scheduled for 21 October 2016.
So while waiting to start her chemo, SF and her husband came to seek our advice.
Chris: In total, so far how much have you spent on your medical treatment?
Husband: It came to about 400 to 500 million rupiah. Something like RM 150,000.
Patient: Our financial resources is drying up. We don’t have much left after this.
C: That is not the end yet, right? You still need to spend more for the radiation, chemo and surgery. And probably more chemo after the surgery.
This is indeed a sad case. After reading all the medical reports, I shook my head in despair. What can I say? What can I do to help? Probably nothing! From my experience over the past 20 years dealing with cancer, I know right in my heart that there is NO cure for cancer. I must be honest with my patients. To help may be possible, but not cure.
My advice to them that morning:
Coming to see us and taking our herbs hoping to cure your cancer is just not right.
Since you have already done 5 times of radiation and are now waiting to go for chemo, why don’t you stick to your planned path — i.e. Go and do the chemo and see what happen.
In the mean time, while you still have a few days, why not read some of my books and understand the “truth” of what you are doing.
After reading, make your own decision as to what you want do. It is okay for me, whether you want to continue with the chemo or not.
For the moment, we shall not prescribe you any herbs. Go home and think first what you want to do.
Comment: This is the first time I have heard of a chemo drug called Kemocarb. From the internet, I learned that this is a platinum-based chemo-drug made by Dabur Pharmaceutical in India. The 450 mg /45 ml drug cost Indian Rupee 2400 or RM 149. Wow, I hope I am right in my calculation! Do you ever wonder why a shot of that chemo cost RM 3,000?
SF story does not end here. Some days later, she and her husband came back to see us again. They decided to forgo further chemo. Why?
This is a sad story, narrated by John (not real name) about his mother’s problem before her death.
CL was a 63-year-old lady. About six/seven months ago, she had abdominal pain and felt bloated. She went to a private hospital and the doctor did an MRI. She was told that it was due to stone in her gallbladder and had to be removed. CL underwent surgery immediately. This procedure cost RM 7,000.
Unfortunately, her problems did not go away. John started to consult some doctor friends who was told him that it was normal. After the surgery, the pains and bloating would not go away immediately. John also asked the doctor who did the surgery why the problems were not resolved. He answered, “There are so many other patients who had the same problems and they did not complain!” The doctor then prescribed medication of gastritis.
In October 2016, CL became very weak and started to vomit and went back to the same hospital again. A CT scan was done and the son was told that shadows in her liver. CL was referred to an oncologist in the same hospital and was told that it could be Stage 4 liver cancer.
Chris: When they removed the gallbladder, did they not check the liver as well?
John: I asked the doctor this question. The answers were: “We only focused on the gallbladder and not any other area during the first time. Also, MRI could not detect liver cancer as easily as the CT scan.”
The oncologist told John that this was a stage 4 cancer and CL had a maximum of 6 months. To confirm, a biopsy was done.
While in the hospital, CL continued to vomit and was put on drip. When she got better, she was discharged; went home and started to vomit again. CL became dizzy and John brought his mother back to the hospital again. The doctor did another MRI. This time he targeted the brain. There was nothing in her brain!
John was told that the cancer was very serious and CL had only 1 or 2 months to live. The oncologist proposed that CL try the oral drug, TS-One.
Chris: Did you take the TS-One?
John: No.
C: Did you ask if TS-One is going to cure your mother?
J: I asked him that question and he did not answer my question. He only said, “Take the drugs for 2 weeks and come back and see me again. And we will see what happen.”
C: Did you ask how much this is going to cost you?
J: No, I did not ask but from the internet I understand that it is expensive.
C: People would tell you that at this point when the patient is at the last stage and is dying, we should not think about money. Money is not important. Do what is necessary. But I think money is important. You do not want to do things just for the sake of doing things — futile efforts with no chance of any positive results.
J: Money is important! But I understand that by giving her the drug, it is going to cause her more problems — the side effects would be severe. There is no quality of life.
(The above is just a gist of our conversation. For more detail, listen to the video carefully. CL died one week after this conversation).
Comments
It is really hard to swallow the idea that when they zoom in on the gallbladder, they could not see or know what is going on in the rest of the surrounding organs! Let’s try to understand a bit of basic anatomy.
The diagram below shows the gallbladder in relation to the liver and pancreas.
The MRI and CT images below show the gallbladder in relation to the liver and pancreas!
According to the images of subsequent careful examinations, we know that from the ultrasound of the abdomen LC had:
an ill defined 3.8 x3.3 x 2.5 cm mass in the left lobe of her liver.
an ill defined 5.9 x 5.8 x 4.9 cm mass in between the left lobe of liver and pancreas.
CT showed more tumours:
ill defined enhancing areas in segments 2,4,5 and 8 of her liver.
ill defined 2.3 x 2.1 cm enhancing areas in the anterior part of the body of the pancreas.
It is not for me to suggest that LC’s problem and subsequent death could be a result of incompetence, carelessness, wrong diagnosis or wrong treatment. It is up to you, those who know how to read, to figure that out. But for one, none of us would want such thing to happen to our own mother. Money gone, suffered and died!
How can we avoid such tragedy? My answer is: Be an empowered patient. Before you undergo any operation, seek a second or third opinion first! Don’t just immediately jump into any hole that you are asked to.
There are three more disturbing events which I think we can learn from this case.
John was told that his mother had Stage 4 cancer, very serious and at most could live no more than 6 months (later reduced to 1 or 2 months). These were masses in her liver and pancreas. She needed a biopsy to confirm this. But, did she really need to do a biopsy? What benefit can a biopsy bring to LC?
Anyway, the USG and CT scan suggested cancer of the pancreas with liver metastasis. Then there is the results of her blood test below:
Total bilirubin
108 H
Direct bilirubin
82.3 H
Alanine transaminase
80 H
Alkalline phosphatase
318 H
Gamma glutamyltransferase
433 H
AST
98 H
CEA
9.9 H
CA 19.9
48,577.12 H
With the above blood test results, ask again: do we really need a biopsy to be performed on a dying person?
LC went home after the biopsy. She started to vomit and later felt dizzy. MRI was ordered. Again, you would want to ask, is this necessary? What benefit can MRI of the brain bring to LC? Yes, there may be brain tumour. But so what if there was a brain tumour? What can we do about it?
After the biopsy result confirmed metastasis to the liver and pancreas, the oncologist suggested LC try TS-One!
Smart of John to ask what TS-One can do for his mother. This is the classical example of the mantra,”Cannot cure but we have treatment.”
Wait a minute doctor, but what is TS-one actually used for? Is this for treating liver cancer and/or pancreatic cancer?
From the internet, we learn that TS-One Capsule is used for the treatment, control and prevention of stomach cancer! Was LC having stomach cancer?
Beside the money — having to pay for the expensive drug, you also need to know that you may be led to buy misery in the form of the following side effects.
When I first read what Dr. Anton Chekhov wrote, I thought it was meant to be just a joke since he was also a dramatist besides being a doctor! Now, with the above story do you see what he wrote may not be a joke? Do you want this to happen to your mother?
The point we want to ask further is, can medical error happen? Yes, it can … more often than we care to admit. Read what Dr. Atul Gawanda and Dr. Paul Ruggieri wrote in their books.
This is an e-mail we received from the brother of a 58-year-old breast cancer patient.
My sister has been diagnosed with breast cancer. The lump on her right breast had been removed on 23 March 2016. Upon strong recommendation by the doctors, first cycle chemotherapy (FEC regimen) was done on 24 April 2016 but due to chemo extravasation, she is now having a deep and large wound with pus on her left arm and needs daily dressing at the hospital, although it is recovering but the rate is slow.
Due to the harsh chemo side effects, we do not want to proceed further with the chemo anymore and decided to consume your herbs. She might not be able to go to Penang for the time being because of the need to do daily dressing for her wound, I am able to see you in Penang if necessary.
The patient’s brother came to seek our help. His sister was supposed to undergo 6 cycles of chemotherapy. But this has to stop because after the first shot of chemo, the injection site in her left forearm developed blisters which later progressed to deep wound (picture) below. It has been more than 2 months and the recovery of her wound has been very slow. Fortunately, the patient did not suffer any pain from the wound.
Comments
It is sad that such a thing ever happened. And I was curious why it could happen! I spent one Sunday afternoon surfing the internet for more information. Problem like this is known medically as EXTRAVASATION.
In my book, Cancer War, I had a picture as below but I would never imagine it could be that bad as the picture above.
Let us do some serious thinking!
If a little of the chemo-drugs leak out and spill onto your unprotected arm and cause such damage, dare you imagine what is going to happen when the drugs get into your body? Honestly, I dare not imagine and also I cannot understand how such a toxic or corrosive drug can ever cure anything.
Imagine again, just a few ml or drops can cause such damage, what could have happened if you pump in a bottle of such toxic drug.
I am amazed. Our blood vessel must be very, very strong and resilient to be able to withstand such corrosive drugs. Yes, they need to pump the drugs into the vein. Surprising indeed the vein does not “rot away” like the picture above.
From the information below, you will learn why such a catastrophe can happen. And such things should not have happened. Also in the literature we learn that such incidence is rarely reported!
Information from the Internet
Extravasationis the process by which any fluid or drug accidentally leaks into the surrounding tissue. In terms of cancer therapy, extravasation refers to the inadvertent infiltration of chemotherapy into the subcutaneous or subdermal tissues surrounding the administration site.
Many cytotoxic agents can cause severe tissue damage if an IV needle or catheter delivers the drug into tissues rather than into the bloodstream. The term extravasation is used when a cytotoxic drug infiltrates into local tissues.
To avoid infiltration the larger veins of the arm are used for IV administration.
Data on the incidence of either extravasation are scant due to the absence of a centralized register of chemotherapy extravasation events.
Incidence rates vary greatly. Estimates between 0.01% and 7% are noted in various publications. Some data suggest that the incidence is decreasing probably due to improvements in the infusion procedure, early recognition of drug leakage and training in management techniques.
In order to minimize the risk of extravasation, the staff involved in the infusion and management of cytotoxic drugs must be trained to implement several preventive protocols.
Should an extravasation occur, it is important to remember that the degree of damage is dependent on the type of drug, the drug concentration, the localization of the extravasation and the length of time a drug develops its potential for damage.
Extravasation is not as rare as many people think, and it may occur even in the most closely monitored situations. A study which investigated extravasation over a five-week period in a UK hospital established an incidence of 39% in adults, almost double that of previously published reports.
Extravasation injuries remain uncommon, with an estimated incidence published in the literature of between 0.1% and 6% in patients receiving chemotherapy.
The published rate is likely an underestimation, however, as many cases of extravasation go unreported.
The true incidence of chemotherapy vesicant extravasation is unclear since there is no central reporting mechanism. With an increasing awareness of the risks from extravasation, the frequency appears to have fallen.
As such, this rate probably underestimates the true incidence of chemotherapy extravasation injury.
Cytotoxic agents have the potential of causing destruction of healthy cells. Due to the relatively low number of cancer treatment centres, it is often not possible for a patient to take the complete course at the centre itself because of financial constraints and long distances from their home towns or villages. After the initial one or two courses, many patients find it convenient to take the remaining treatment at their nearest health institution. However, physicians in such nonspecialized centres may not be aware of the local side effects of the drug. Very often, even in oncology hospitals, the work of infusion of cytotoxic drugs is left to a junior house surgeon or an intern, whose inexperience in venupuncture and ignorance of precautions for infusing a cytotoxic drug can lead to extravasation of the drug.
Extravasation of the drug can produce extensive necrosis of the skin and subcutaneous tissue. This not only adds to the misery of the already seriously ill patient, but can also cause serious functional loss, as most often, the forearm and hand veins are used for infusion.
This study was done in the Department of Plastic Surgery of a Medical College in the period from January 2002 to December 2006. There were twelve patients. All the patients were from rural areas and belonged to lower socioeconomic strata. None of the patients was educated beyond middle school.
Mitomycin C was used in seven cases (58.33%), vincristine in two cases (16.66%), 5-Florouracil in another two cases while doxorubicin was responsible for extravasational side effects in one case (8.33%). The size of necrosis ranged from 3.75 cm2 to 25 cm2 with average area of 9.6 cm2 [Picture below].
In terms of the area involved, the dorsum of the hand was involved in five cases (41.66%), the wrist in another five cases (41.66%), and the cubital fossa in the remaining two cases (16.66%).
Extravasation of cytotoxic drugs leads to symptoms which are self-explanatory for this catastrophe. The majority of the patients will complain of excruciating pain and itching in the infusion site. Within a few hours, the extravasation area will show erythema, edema, and induration. Within a few days, these signs and symptoms will increase and the skin will show discoloration and desquamation of the epidermis or blister formation will follow. If a large dose of a cytotoxic drug is extravasated or no intervention is taken at this step, the area will show ischemic changes and ulcer formation will be inevitable.
It is well said, “Prevention is better than cure” and this holds true for extravasation injuries also. Once there is an extravasational injury to the tissue, morbidity is inevitable. Extravasations of cytotoxic drugs further increase the suffering of cancer patients. This catastrophe can only be avoided by vigilance.
Use of chemotherapeutic drugs is commonly associated with substantial complications. These drugs are infused in veins of dorsum of hand or antecubital fossa.Subcutaneous extravasation is a known complication of intra-venous administration of chemotherapy agents. There are limited cancer centers throughout the globe with properly trained medical professionals. Due to lack of specialized centers and experienced medical professionals, chemotherapy infusions can lead to higher incidence of extravasation injuries. The overall incidence of extravasation injuries varies from 0.1-7%. It is characterized by drug escaping out of the vessels in subcutaneous tissue plane due to repeated venous punctures and its cytotoxic effect of the chemotherapy drug. The infusion area over dorsum of hand is having minimal subcutaneous fat tissue and so it is more prone for severe damage by extravasation injuries; this injury can damage underlying tendon, joint, and neurovascular structures.The extravasation injuries are difficult to treat due to lower immune status of the patient and complexity of the wound with exposed bone or tendons.
At our center over 3-years period, 32 patients were treated for chemotherapy extravasation wounds. Out of these 32 patients, seven had wound over dorsum of hand. Two patients were treated with chemotherapy for carcinoma lung. Other patients were of Non-Hodgkin’s lymphoma, Osteosarcoma, Breast carcinoma, Oropharanyx carcinoma, and Brain tumor.
Cyclophosphamide was used in four patients (81%), Doxorubicin in three patients (43%), Adriamycin in two patients (28%). Vincristine, Prednisone, Cisplatin, 5 Flourouracil, Adriamycin, Cyclophosphamide, Docetaxel, Procarbazine, Vincristine, Lomustine was responsible for extravasation injury in other patient.
This is a tragic story which I find it real hard to “understand.” WF is 32 years old. In early 2014, WF felt a lump in her left breast. At that time she was pregnant and was about to deliver her baby. So nothing was done until after the birth of her baby.
On 14 March 2014, WF had an ultrasound of her breasts. “There is a 17 mm x 9.6 mm lesion at 2 o’clock position of left breast, 4 cm from the nipple.” A FNAC (Fine needle aspiration cytology) done in a Taiping private hospital showed “benign breast lesion.”
WF did another FNAC in April 2014. This time it was done in a private hospital in Penang. Unfortunately, the result showed “atypical cells … Highly suspicious of an infiltrating duct carcinoma.”
A trucut biopsy was done on 12 April 2014 confirmed an invasive ductal carcinoma.
WF consulted another doctor in another private hospital.
25 April 2014Ultrasound of Both Breasts
Irregular hypoechoic lesion between 1-2 o’clock. It measures 23 x 18 x 12 mm. Some microcalcifications seen. In keeping with a neoplasic lesion.
Based on the above, WF had surgery. A wide local excision of the left breast mass was done (lumpectomy). The tumour removed was 23 mm in size. Two of the axillary lymph nodes were involved. All resection margins were free of malignancy. Immunohistochemical study indicated a triple negative tumour: ER negative, PR negative and c-erb-B2 negative. It was a Stage 2B cancer.
9 May 2014Ultrasound of Thyroid
Multiple tiny nodules seen on both thyroid lobes, likely benign.
WF subsequently had 6 cycles of chemotherapy. Neither she nor her husband knew what drugs were used. Anyway, each cycle cost RM 6,000. WF lost her hair, felt tired and nauseous during her treatment. Chemotherapy was completed by October 2014. Then WF received 20 sessions of radiation and this was completed in November 2014.
About a month later, in late December 2014, the cancer spread to WF’s brain. There were 3 lesions in her brain. WF received 2 sessions of radiation to her head in January 2015.
Two months later, March 2015, CT scan showed the cancer had spread to her lungs, bone and liver.
WF was again asked to undergo 4 cycles of chemotherapy. WF did one cycle after which she and her husband came to see us and decided not to proceed with the treatment.
Chris: Did you ever ask the doctor if surgery, chemo and radiation were going to cure your cancer?
Husband: The doctors said there is a 80 percent chance of cure?
Chris: Did you ever ask what happen to the remaining 20 percent?
No reply.
Study the numbers of her blood tests.
Date
CEA
CA 15.3 (normal 0-32)
5 June 2014
Less 0.5
12.3
18 Nov 2014
0.4
9.7
10 Feb 2015
Less 0.5
13.2
10 March 2015
n/a
20.3
24 March 2015
n/a
37.0
7 April 2015
n/a
96.1
22 April 2015
1.4
142.6
In March 2015, WF was started on chemotherapy again because her CA 15.3 started to rise, indicating that the earlier chemotherapy had failed. Therefore, the answer is more and more chemo?
The following are results of her CT scan and MRI.
Before chemotherapy
9 May 2014CT scan of Brain, Neck, Chest, Abdomen and Pelvis
Recent wide local excision of left breast carcinoma and left axillary clearance.Brain: There is no shift in the midline structures of the brain. No mass or abnormal enhancement. No extracerebral fluid collection.Lymph nodes: There are no enlarged supraclavicular, axillary, internal mammary, mediastinal or pulmonary hilar nodes.Lung: There is no pulmonary nodule or other significant pulmnary abnormality.
Liver: Liver parenchymal density is normal. Two small hypodense lesions in segment 8, both measuring 4 mm and another two hypodense lesion in segment 7, both measuring 3 mm. Likely represent small cysts.
Bone: no significant lytic or sclerotic bone lesion seen.
After chemotherapy
9 January 2015MRI of brain
Bilateral cerebral metastases.Left frontal cortex – 21 x 16 x 15 mm well defined multilobulated massLeft basal ganglia – 9 x 8 x 9 mm.Occipitotemporal cortex – 8 x 8 6 mm.
Lesions also associated with perilesional oedema.
10 January 2015CT scan Neck, Thorax and Pelvis
There is no evidence of local recurrence.Interval development of a few small lung nodules within the right lower and left upper and lower lobes. They are too small to characterise but may represent secondary deposits.Apical region of left upper lobe – 3 mm noduleRight lower lobe – 3 mm nodule
Basal segment of left lower lobe – 4 mm nodule.
10 February 2015MRI of brain
Partial regression of bilateral cerebral metastases.Left frontal cortical lesion – 11 x 8 x 10 mmLeft basal ganglia – 7 x 6 x 5 mmRight occipitotemporal cortex – 6 x 5 x 4 mm
There is no associated perilesional oedema.
No new nodule seen.
24 February 2015MRI of brain
Cerebral metastases increased in size.Left frontal cortical lesion – 17 x 11 x 15 mmLeft basal ganglia – 8 mmRight occipitotemporal cortex – 9 mm
Perilesional oedema has also increased.
24 March 2015MRI of brain
Cerebral metastases minimally increased in size. Reduced perilesional oedema. There are likely post radiation changes.Left frontal cortical lesion – 16 x 13 x 16 mmLeft basal ganglia – 8.3 x 8.0 mmRight occipitotemporal cortex – 9 x 9 mm
7 April 2015CT scan Neck, Thorax and Pelvis
Increased size of pulmonary metastases. Interval development of hepatic and skeletal metastases. And mild retroperitoneal lymphadenopathy.Lung: Apical region of left upper lobe – 4 mm nodule with central cavitation.Right lower lobe – 4 – 5 mm noduleBasal segment of left lower lobe – 4 – 5 mm nodule.
Liver: Numerous small hypodense lesions inn both lobes of liver. Larger lesions measuring up to 15 mm.
Lymph nodes: Multiple mildly enlarge para-aortic lymph nodes – measuring up to 12 mm. Smaller lymph nodes are present along the aortocaval space.
Bone: There is an irregular poorly defined lesion in the manubrium sterni eroding the bony cortex. There is also suggestion of similar lesions in the lower cervical spine.
We need to acknowledge that the oncologist did a “good” job of taking the base line of WF’s health before chemo and radiation were started. Yes, before the treatments, WF’s brain, lymph nodes, lung, liver and bone were all clear! Meaning at that point in time, her cancer did not spread anywhere! So the doctor confidently told WF and her husband that there was a 80 chance of cure!
Then chemotherapy and radiotherapy were started.
Barely a month after treatments were completed, problems started to show up.
First, the brain. There were 3 metastatic spots in the brain. There was no such tumour before right?
Radiation was given to the brain. The tumours shrunk a bit — by just a bit — and then started to grow again.
By end of March 2015, WF’s CEA started to increase telling us that chemotherapy / radiation had failed.
Then, more chemo was suggested. WF had one cycle of this second-round chemo.
In April 2015, CT showed the cancer had spread to her lung, liver, lymph nodes and bone, besides the brain.
Sores causing difficulties to eat
Brain and lung
Liver
Ask these questions.
April 2014 she was diagnosed with a 2 cm malignant breast lump. A year later, April 2015, the cancer had spread to her brain, lung, liver, lymph nodes and bone. She did surgery, chemo and radiotherapy as dictated by the doctors. How could this be? Why do the treatments when the cancer cannot be contained or cured?
Dare you ask, what if WF were to do nothing? Just leave the lump as it is. Would she end up the way she is now – with more cancer all over in the body?
Is WF’s case unique or exceptional? There are many more tragic stories like this. Here is another example, click this link: Does chemotherapy make sense?
Some people may wish to say this is a triple negative cancer. So it is an aggressive type! Some people may say it is just your luck! My response: Many patients live a healthy life by making a CORRECT choice!It is your life.
Jane had a 1.2 cm lump in her right breast. Like WF above, she did a lumpectomy. Her tumour was a double negative type — negative for ER, negative PR but strongly positive for c-erbB-2. P53 was strongly over-expressed.
Jane was told to undergo chemotherapy. The package of chemotherapy + Herceptin would cost RM 120,000 while radiotherapy cost an additional RM 35,000. Jane was told that the benefit of chemotherapy and radiotherapy would be 16 percent – i.e. 16 out of 100 women are alive and without cancer because of the combined therapy.
To Jane the benefits of chemo and radiation did not make sense. She promptly refused further medical treatments and came to seek our help on 10 January 2010.
Jane told us that she refused chemotherapy because she did not want to lose her hair. In addition, her mother-in-law had lymphoma and died after two cycles of chemotherapy.
This is the story of a 66-year-old lady who had lung cancer. The cancer has spread to her lymph nodes, bones and brain.
This is what her daughter wrote about her mom.
Mom who cooked and ate meat, dairy, eggs, honey, garlic and onion as part of her diet since young, became a vegan since 3 years ago when she started to follow Master Ching Hai’s teachings.
Mom had high blood pressure for about a decade now. She used to take medicine to control her blood pressure but has since stopped taking it about 6 months now. Mom is a non-smoker.
Since June 2013, mom started to complain about being tired and she slept a lot. She felt no mood or lazy to do housework. We thought all these were due to aging. She also tended to forget things, like misplacing items.
Sometime in early August 2013, she lost her balance and fell. Mom declined to see the doctor.
Mom started to look very tired. She also had a hard time formulated her speech and stammered. She started to take vitamin B12 pills in the hope of improving her condition. We all thought she might suffer from vitamin B12 deficiency being a vegan. Mom wanted to monitor for 2 weeks before seeing a doctor.
Walking extremely slow, one step at a time, and very tired, we brought mom to see a GP. The doctor advised blood test together with a CT scan at a hospital. The doctor suspected a minor stroke.
Mom Had Cancer
We brought mom to a university hospital. Her CEA was more than 1,000. She was referred to an oncologist who suspected mom had cancer. He prescribed mom Dexamathasone, to reduce swelling of the brain and Omezole – to take care of the side effects of the steroid medication.
CT/PET scan on 3 September 2013, confirmed that mom has Stage 4 lung cancer. The cancer had spread to her brain, mediastinal nodes and bones. The next day, she did a biopsy. The tissue was positive to EGFR.
Radiotherapy and Iressa
From 11 to 23 September 2013, mom had 8 session of radiation treatment to her brain. From 21 September to 11 November 2013 (about 7 weeks) she took Iressa.
Deceptive Positive Results
A second MRI and PET scan was done on 13 November 2013. The results were great! Mom’s brain metastases reduced tremendously. Also the lesions in her lungs shrunk.
However, liver function test taken on 11 November 2013, indicated liver damage.
Mom had to stop Iressa.
Another blood test on 9 December (i.e. 3 weeks after stopping Iressa), indicated liver got better. Mom started to take Iressa again. This time, a table on alternate days. But in January 2014, mom started to take Iressa daily.
More of Deceptive Positive Results
During the Chinese New Year (February 2014) mom started to lose her voice. A third MRI/PET/CT scan was done on done. The results were:
The oncologist was pleased with the MRI result. The oncologist mentioned that in September 2013 MRI there were about 50 lesions in her pain. In this February 2014 MRI showed less than 10 lesions. The oncologist said when he first saw mom’s MRI, he did not think mom was going to make it.
However, the PET scan results showed a different story. In the September 2013 PET scan it was a nice result with much reduced lesions (almost not seen). But for this February 2014 PET scan results, some lesions had recurred near her right neck (near vocal chords — therefore loss of voice?).
The oncologist mentioned that he was very worried, “it looks like the cancer cells got smarter and tried to overcome the Iressa.” Mom was asked to continue with her Iressa.
The oncologist, however, suggested a few options:
1. Start chemotherapy on day 1 and day 8, then rest for 3 weeks. In addition, mom take another oral drug, Tarceva or Afatinib (which was recently approved and is now available for free). We told the oncologist that we preferred not to do chemotherapy. As such the oncologists suggested the following options.
2. Start radiotherapy to the body in addition to taking another type of oral drug similar to Iressa.
3. Take only Tarceva or Afatinib without chemotherapy. But the oncologist said this was not a viable option.
For mom’s voice issue, we brought mom to see an ENT specialist. Endoscopy to the nose/throat showed the left vocal cord was not moving (paralysed?) but the right one was doing fine. The ENT specialist said the problem could be due to the cancer. There is no medicine that he could prescribe for mom.
March 2014 — Iressa failed, switched to Tarceva
Blood test on 5 March 2014, showed the tumor markers were slightly higher. The oncologist said he was worried that the cancer cells were growing and spreading. He suggested chemotherapy. He said he would give mom a lower dosage, perhaps 80 percent strength instead of the normal 100 percent strength. However there will be side effects such as low white blood cell count but the doctor said this can be countered by taking medicines. He also mentioned that patients can get better after going through the “weak” phase.
As we were reluctant to undergo chemo, the oncologist suggested radiation treatment to the neck and the left side of the lung. This treatment cost RM 9,100. Mom received 10 sessions of radiation.
The oncologist switched mom to Tarceva since Iressa doesn’t seem to be effective anymore. Tarceva cost RM 8,000 per month while Iressa cost RM 7,000 per month.
On 24 March 2014, mom received her fist xGeva (denosumab) injection to protect her bones. This cost RM1,600 per shot and mom is supposed to have it every month.
28 March 2014, mom started to lose her appetite.
April 2014 — 9 months Later
Blood test on 7 April 2014 showed mom’s calcium level had gone down a little due the previous xGeva injection. She was prescribed medicine to bring up mom’s calcium level.
Mom was having frequent bowel movements. The oncologist said this might be due to the side effect of Tarceva, which causes minor diarrhoea.
Mom still had coughs and still choked when drinking fluid. The throat was dry and her voice hoarse. Her appetite was poor.
At this point, we discussed chemotherapy with the oncologist.
1. What after one session, we decided to stop the treatment. Any side effect / problem?
Oncologist: Of course we can stop at anytime, no problem.
2. How does the treatment work in terms of session, timing and rest period?
Oncologist: Do chemo on day 1 and 8 and this is considered as one cycle. Do 3 cycles first.
3. Drugs to use?
Oncologist: Two options. One, Carboplatin + Alimta which is more expensive, costing around RM 8,000 per cycle. Two, Carboplatin + Gemcitabine which cost about RM 1,000 per cycle. This option is much easier on patients but may be less effective (?). It it would be Carboplatin + Gemcintabine, the oncologist suggested that mom go for 4 to 6 cycles.
May 2014 — Tarceva Failed
5 May 2014, we told the oncologist about mom’s side effects. The oncologist recommended to stop Tarceva for 4 days and we were asked to come and see him again after that. He prescribed medications for insomnia, itchiness, and inflammation.
9 May 2014, after 4 days not taking Tarceva, mom got much better. Acnes on scalp were drying up and there were not more rashes. But there seemed to be a new growth at mom’s neck. Oncologist asked mom to take Tarceva again but on alternate day.
MRI on 19 May 2014, showed disease progression. There were about 7 tumours.
PET/CT scan on 21 May 2014, showed disease progression:
1. Lymph node at the neck has enlarged.
2. Few new lesions at T9.
The Final War Plan
The oncologist laid out the following options.
Tackle the brain first – and fast! He recommended that mom go for Cyberknife and then followed up with chemotherapy. After that mom continue taking the oral drug again after 4 months. If mom’s backache persist then we need to give radiation to that location.
The oncologist also explained that giving mom whole brain radiation again would cause more side effects (e.g. sleepy, headaches) and only low radiation dosage could be give. If mom’s goes for Cyberknife she shouldn’t have such side effects because Cyberknife is more targeted.
Cyberknife cost RM 67,000.
Another option is to go for chemotherapy first. Do MRI after 1 or 2 months and if the tumour is shown to be growing very fast then go for Cyberknife.
The oncologist assured us the mom would be able to tolerate chemotherapy. The only thing we need to really watch out is the white blood cell count.
Mom will have to continue with her monthly xGeva injection to strengthen her bone.
One Final but Most Important Question
Can all these treatment cure mom?
The answer is: No cure. There is no guarantee that the cancer will not recur even after Cyberknife.
CA Care – the Last Resort, 23 May 2014
Patient came to seek our help and was prescribed herbs. On 8 June 2014, patient and her husband and daughter came to CA Care Penang and underwent the e-Therapy for her pains.
Comments
As I was about to upload this story, I received an email from Singapore. This is what it says.
Dear Mr Teo,
My husband, age 61 was diagnosed with lung cancer 2 years ago. He was on Iressa since last year September 2013. Two months ago the oncology asked him to start chemo as he has developed tightness in the chest. We decline. So we just have to carry on with Iressa. Two weeks ago he developed bloatedness in the stomach with wind and fluid. Again oncologist scheduled him for chemo this coming Monday. Currently he feels very fatigue and is too weak to go for chemo cause he lose a lot a weight.
We are not in favour of chemo because in year 2012 he had gone through that already and we find it is too damaging to the lung and show no result because 10 months later lung had fluid.
It is indeed sad.
Don’t those who are supposed to know, know that Iressa does not cure any cancer? And chemo does not cure lung cancer either? Click this link: https://cancercaremalaysia.com/category/lung-cancer/ and you will see that I have written no less than 70 stories about lung cancer and chemotherapy / Iressa / Tarceva, etc.
Can we not learn something from these stories?
More stories about this patient:
Lung-Bone-Brain Cancer: Pain Gone After 4 Days of e-Therapy
Lucy (not real name – H974) is a 52-year-old female. She was diagnosed with ovarian cancer in March 2011 and had undergone a TAH-BSO (Total Abdominal Hysterectomy Bilateral Salpingo Oophorectomy) at a private hospital. The medical report indicated the following:
A huge single right ovarian cyst 15 to 18 cm
Intact capsule
No ascitis, no peritoneal / omentum / liver deposit
Lateral pelvic wall clear
No adhesioin
Left ovary normal
Both fallopian tubes normal
Clear cell carcinoma of right ovary, Stage 1
Lucy was asked to undergo follow up chemotherapy. She declined. She said, I did it my way and went for traditional method. She embarked on taking Sabah Snake Grass (SSG) since much has been said about its goodness in the local mass media. Lucy started with 300 leaves but when she began to have joint pains, she reduced the consumption to 30 leaves each time. Lucy had been taking this fresh herbs for more than a year – from May 2011 until September 2012 (when she came to seek our help).
Recurrence: Extensive spread
In May 2012, Lucy had lower abdominal discomforts and did an USG. The result indicated a possible presence of a mass in the Pouch of Douglas. The echodensity measures 3.3 x 3.6 x 5.2 cm. She went to consult three doctors.
Doctor 1 said there was nothing wrong! No mass.
Doctor 2 said there was something in there but unsure of what it was!
Doctor 3 also said the same – something in there!
Knowing that her cancer had recurred, Lucy started to take the SSG again and this time more seriously at 300 leaves each time.
Eventually Lucy ended up in the government hospital performing a CT and PET scan. The results of the CT scan indicated:
a heterogenous mass – 5.3 x 4.0 x 4.4 cm – at the pelvis suggestive of tumour recurrence.
possible infiltration into the adjacent sigmoid colon and right pelvic nodal metastasis.
enlarge lymph node along the right pelvic – largest 1.9 x 1.1 cm.
the peritoneal soft tissue nodule – 1.4 x 1.2 cm – may represent peritoneal metastasis.
Comment
Sabah Snake Grass (SSG) is not new to me. I know this plant since 1995 when I started CA Care and has been using it as one of the 350 herbs used in our centre. However what is new to me is the idea that only ONE herb is used as if it is a magic bullet. This unfortunately is against the basic principle of herbal therapy. Nevertheless this is what happened when one has a “magic bullet” mentality.
Over the years, I receive emails from people asking for my opinion about this “hot” topic of SSG. See below:
Hi Dr. Chris, recently I read from newspaper regarding Sabah Snake Grass (Clinacanthus) herb which can help in cancer treatment. Do you have any comment on this … for cancer?
Good News!!! Recently, I met a man who had Lymphatic Cancer – Stage 4 with lymph nodes affected. His cancer started in March 2008.
Affected parts: 1st: Right lung, 2nd: Left lung, 3rd: Groin, 4th: Eye and 5th Mouth. After 9 chemo therapies he stopped the treatment on 10/11/2008 because 5 specialists said he can only survive for 3 months. Today, after more than 2 years, he has recovered and is still living.
Thanks to the Sabah Snake Grass (Clinacanthus) which he planted outside his house. He blended the leaves with green apple (minus skin and seeds) and drank them after breakfast every day.
After 3 days, 6 tumours disappeared. After 13 days, he went for a blood test. The oncologist said that he was 96% cured. So far more than 200 people who had taken the herbs showed improvement.
Case 1) Man – age 54, LungCancer: 3rd stage. Chemotherapy 6 times. Tumour before taking Sabah Snake Grass 29mm, 44mm, 76mm. Tumour two weeks after taking Sabah Snake Grass reduced to 20mm, 27mm, 67mm respectively
Case 2) Woman with Uteruscancer – tumour size 6cm Scheduled for surgery. After taking SSG, reduced to 3.5cm. Doctor said no need to operate. Continue taking the SSG, the tumour disappeared.
Case 3) Man with ProstateCancer.
After taking SSG for 11 days, the tumour disappeared.
Case 4) Woman from KL, Breast and LungCancer
Both breasts removed – 4 stage. Very weak, cannot eat, on drip and lying in hospital. Family member poured SSG juice into her mouth through tube. After a few days, could eat and was discharged. 28 days later was all tumours disappeared.
Case 5) Woman from Taiping with Breast Cancer After taking SSG for 3 days, the wound dried up.
Case 6) Leukemia Patients So far 4 cases have been cured after drinking SSG juice. They also drank juice from 3 leaves of Guo Sai Por (Ti Tham Tou) once per week.
This was my reply to the person who wrote me:
Scientists in Thailand have been studying this plant. There is also a company making cream from this plant. I also grow this plant in my garden for many years already. I also use this plant for cancer but not in the way it is being publicised much less getting “instant, magic” results as claimed.
Does the plant really cure cancer like written above? I HOPE IT IS TRUE … but I am not sure and it is very, very difficult for me to believe such stories without clear, hard evidence. Let me say it clearly: I want to believe these stories but I cannot. My training as a scientist just tell me it does not make sense – they are too good to be true. As a scientist, I also find such claims more of a “joke.” Nobody with a scientific mind would be able to swallow such success stories as the way these are written! Let me say it here — I am not saying they are not true but what is questionable is the way the stories were written and presented. I am sorry to say this but I still have to say it. But unfortunately many of us only want to hear what we want to hear, throwing away logic and common sense out the window.
In this video, a lady related her experience with SSG. She had been taking it for over a year and she suffered a recurrence. SSG could not even prevent a recurrence let alone make tumours disappear.
The above patient is not the only one who experienced such failure. I have many others who came with similar failed stories. I have also personally given SSG to a lady with small lumps in her breast. The leaves were harvested from the plants that I grew at home. I asked her to take the juices every day. It did not work. She had to go for chemotherapy.
Let me be clear about this. I am not against anyone taking SSG. By all means take it if that makes you happy or feel good. Take it if you benefit from it. You could be the lucky one. After all you don’t have to sell your house to pay for the herb. So there is nothing much to lose. But if you have problems after taking it, you may want to stop taking it. Some patients told me that they experienced joint pains or muscle cramps and could not walk after taking SGG. Again, this can happen to some people, while others have no problem.
To those of you out there. Let me know if you have any good healing stories about SSG. As a reminder, whenever we want to make any claim of efficacy, we must present our case with a certain degree of credibility. Our story must be substantiated by medical reports, CT scan, blood tests, etc. Let us document such success stories properly so that others would not laugh at us. Shoddy work makes us look cheap! We give others all the reasons to say we are quacks. Let us do our work correctly!
According to the above stories, you need to take SSG for only 3 days, 14 days, 11 days or 28 days and the cancer all disappeared. Wow, Malaysians have “beaten” all American scientists at curing cancer with a magic bullet!
The file of KT (S346) was on my table. She was a 42-year-old Indonesia lady who had been battling with her breast cancer for about 12 years. I was taking my time wanting to write her story. But today, 29 May 2013, I received this e-mail from her husband.
Dear Madame Beng Im , Dr. Chris Teo, Dengan sedih dan menyesal kami informasikan bahwa KT sudah meninggal dunia Selasa 21May at 02.55 a.m. (early morning). Dan sudah dimakamkan Kamis 23May, at 11 a.m.
Friday, 17 May kesehatan drop, makan dikit/tak ada selera , minum obat herb tea juga tidak mampu. Monday 20 May at night, so weak. We carry to hospital. Dokter said that she was in bad condition, no hope. She just stayed in hospital 1night only. Tuesday 21 May, at 02.55 she was gone / dead. Many thanks for CA Care’s support for my wife.
About two months ago, 22 March 2013, KT and her husband came to seek our help. She stayed in Penang for almost a week. This was her tragic story.
About one and half years after her second child, KT found a 1.8 cm lump in her right breast. On 16 May 2001 a biopsy was performed and confirmed that it was malignant – a ductal carcinoma, positive for estrogen and C-cerb-B2 receptors but negative for progestrone.
On 19 May 2001, KT underwent a lumpectomy at a cancer hospital in Jakarta. It was a Stage 1 cancer. From June to October 2001, KT received 6 cycles of chemotherapy, followed by 25 sessions of radiation treatment in November to December 2001. She was not prescribed any medication.
About three years later, 12 July 2004, the cancer recurred at the previous operation site. A biopsy confirmed it was a ductal carcinoma again. USG and bone scan were performed. No metastasis was detected.
On 21 September 2004, a mastectomy of the right breast was performed at another hospital. And this was followed by 20 radiation treatment. The doctor suggested ovarian ablation and more chemotherapy but KT refused the treatment.
About five years later, in 2009, the operation site developed an open wound with recurrence of cancer around the wound. USG and bone scan on 20 November 2010 did not show any metastasis.
On 3 December 2010, a biopsy was performed of the regrowth and histology indicated lobular carcinoma. The doctor suggested chemotherapy but KT refused the treatment. She did nothing after that.
In June to August 2011, KT went to China for treatment. PET/CT scan showed the wound was 14 x 12 cm and the cancer had spread to her lymph nodes, lungs and bone. This was a Stage 4 cancer.
In China, KT received the following treatment:
10 June 2011:
Patient received iodine seeds implantation and cryosurgery in the lung,
Iodine seeds implantation in the axillary fossa metastatic lymph nodes.
17 June 2011: Patient received recurrence tumour resection, dermatoplasty and PDT (photodynamic therapy).
16 July 2011: Patient received re-dermatoplasty in the back ulcerates.
15 June to 23 June 2011: Patient received DC-CIK immunotherapy.
20 September 2011: Patient received re-dermatoplaty in the back ulcerates.
27 September 2011: Patient received iodine seeds implantation in the scapular region and left costal bone.
KT was again asked to undergo chemotherapy. She again refused the treatment. But she agreed to take Tamoxifen.
On her return to Indonesia, KT started to seek out alternative therapies. She tried sour sop leaves, Mahkota dewa, benalu kopi, etc. She also tried radiofrequency jacket.
On 22 March 2013, KT and her husband came to seek our help.
Comments
When I saw the picture of her breast, I must say I was terribly upset. How could such a thing happen? The first thing that came to mind was, Was this not a work of a bomoh or quack? After all, too often we read in the newspapers that things like this only happen to patients who go and seek the help of alternative healers. But no, the reality was that she sought medical help from the very beginning after discovering a 1.8 cm lump in her breast. And mind you, it was an early stage cancer – Stage 1. I could not understand how she could end up like this.
What can we learn from this tragic episode? Ask these questions:
Is medical treatment of cancer really that proven or scientific?
When you have cancer – can you really achieve a cure?
What could have happened if she were to take a non-medical route?
Robert G. Wright, founder of the American Anti-Cancer Institute wrote in his book, Killing Cancer Not People:
Slash, Poison, Burn. The Big Three. What you probably don’t know is that they have no possibility of healing your cancer. Let me repeat that. They haveabsolutely no possibility of healing your cancer. They actually cause cancer.
The saddest and most tragic part of all is that we’re not only dying of the “disease” now, we’re dying from the treatments. Cancer cannot be cured with drugs, surgery, chemo or radiation; not now, not ever, not possible.
When it comes to cancer, your doctor / oncologist will fail you.
It is up to you what you want to do with the above statements by Robert Wright. Looking back over the 16 years helping cancer patients, I must say such episode happen often enough. It is NOT unusual or exceptional.
AS (S-357) is a 65-year-old Indonesian. He came to seek our help on 14 April 2013 after having undergone a failed liver surgery in Singapore.
His problem started in late December 2011 when AS felt gastric-like pain in the stomach. An ultrasound at a hospital in his hometown indicated a possibility of gallbladder infection.
Not satisfied, AS went to Jakarta and on 31 December 2011 underwent a cholecystectomy (surgery to remove gallbladder). During the operation, the surgeon also did a liver biopsy for suspicious liver lesions.
In February 2012, AS went to the National Cancer Centre in Singapore for a second opinion. The histology slides from the early surgery and liver biopsy were reviewed. The liver biopsy showed poorly differentiated tumour.
A whole body PET / CT on 2 February 2012 revealed left hepatic lobe mass, measuring 3.2 x 2.6 cm (picture below).
On 25 April 2012, AS had another CT scan. The report indicated interval increase in size of the dominant heterogenous hepatic mass from previous 2.9 x 2.6 cm to currently 0.3 x 3.5 cm. No other new focal hepatic lesion seen. (Note: this report stated a different tumour size compared to the earlier report. A mistake somewhere?).
On 3 May 2012, AS underwent a hemihepatectomy – i.e. a surgery to remove one-half or a lobe of the liver. The tumour was at the left lobe of his liver. AS was discharged on 9 May 2012. The procedure cost S$28,000.
Liver histology indicated a hepatocellular carcinoma (HCC or liver cancer), 4 cm, Edmondson Grade 3 with 3 satellite nodules. Resection margins were clear. Vascular invasion was present. The 2 diaphragmatic nodules were metastatic HCC. Gallbladder shows chronic cholecystitis with no malignancy seen within.
About three months later, 16 August 2012, AS went back to Singapore for review. A repeat CT of abdomen and pelvis showed NO evidence of recurrent HCC or focal liver lesion.
Unfortunately this euphoria did not last long. Six months later (i.e. about 9 months after the surgery) another PET /CT scan on 11 March 2013, revealed a new recurrent hetergenous hypodense mass in the liver at the resected margin measuring 8.0 x 4.8 cm (picture below).
On 22 March 2013, AS underwent TACE (transarterial chemo embolization) for his recurrent liver tumour. Unfortunately this procedure failed. The interventional radiologist was unable to access the tumour feeding vessel. So TACE could not be completed and the chemo drug not delivered. In spite of the failure, AS had to pay S$5,000 for the procedure.
AS was discharged on 25 March 2013 and was referred to an oncologist for chemotherapy. AS decided to give up further medical treatment and came to seek our help on 14 April 2013.
While talking to AS, his wife and son I posed this question: Why don’t you want to go for chemotherapy? After all AS had willingly undergone surgery and TACE – why chicken out now?
The wife replied, We are scared!
AS replied: The doctor did not show any responsibility.
My reply: What do you expect from the surgeon? What more do you want him to do? His job is to cut you. And has cut you and there is nothing more that he can do. He has done his job. Now, he is passing you to the oncologist because he is a surgeon and not an oncologist!
From his reply I fully understand how AS felt – being let down by the surgeon. He was totally disappointed. He came to the surgeon in Singapore believing that he was in the safe hands of the expert. He was willing to pay S$28,000 for the surgery but he did not get what he had bargained for. Now, he was passed on to another doctor – where is the responsibility then?
Let me tell you – AS is not the only one who felt let down or cheated. There are many, many others who come to us with a similar story. I am reminded of one really pathetic case. A man from Pontianak was pushed into undergoing surgery for his liver cancer (see A great failure and let down ) He was told that his condition was serious and surgery must be done immediately. The wife said: The surgeon even hugged me and assured me – Don’t worry, he (my husband) would be well and alright. Oh, it was so sweet of him. Unfortunately after the surgery, the cancer recurred. The patient and his wife tried to seek clarification from the surgeon. They were snubbed. The surgeon did not even want to talk to them. The wife was full of tears when she related this story.
Yes, I fully understand how patients feel after a medical failure.
I told AS and his family that his is a big problem and I am not sure if I could help him. I can only do my best. AS was prescribed Capsule A, B, C and D. In addition he has to take LL-tea, Liver 1 and 2 teas. We sent him for a blood test. The results as of 15 April 2013 showed his alpha-fetoprotein = 1,064.0 and total bilirubin = 25.0. Other liver function enzymes were within normal range.
Question You Should Ask: Can surgery cure me?
I always pose this question whenever a patient comes to see me, Before you undergo surgery, chemotherapy or radiotherapy, did you ever ask the doctor if the treatment he is giving you is going to cure you? You will be surprised most cancer patients don’t ask such question. They take it for granted that they will be cured!
AS told me. I did not ask that question. I only asked, What is the best way out for me! I told him, That’s the wrong question to ask! If you go to a barber, he will tell you the best option for your head is to cut your hair. If you ask a hammer what all of us look like in this world, the answer would invariably be, You all are nails meant to knocked down! You go to a surgeon he would most likely say, Operate. That’s his best option for you. Ask the oncologist, he would invariably say, Go for chemo! You have missed the point here. Isthe procedure suggested going to cure you? This ought to be the main concern.
By asking the wrong question, you get an answer that brings you elsewhere – perhaps where you don’t want to go. So, my advice to all patients, Ask this all important question – can your treatment cure me? Don’t be afraid, ask.
After you get the answer then use your commonsense to evaluate what the doctor tells you. Does it make sense? Do you believe in the statistics or percentage or whatever claim the doctor gave you? If this is not what you are looking for, go elsewhere. Look for another path.
Likewise, when you come to CA Care and tell me that you want me to cure you of your cancer I would tell you this, Go elsewhere – I don’t have the magic bullet and I cannot cure you! In my many years helping cancer patients I don’t really see any so-called cure for cancer. Cure means the disease goes away and never come back. Generally, the cancer recurs after some years. My auntie died of metastatic cervical cancer after an apparent cure, 13 years later! Where is the cure?
In the case of AS, surgery did not cure him! After 9 months, the tumour grew back and this time it grew more than twice its original size. Where is the cure?
The next question you probably need to ask is about your diet. This question will give you some idea about the kind of doctor you are dealing with! His answer shows his perception about health in general. And more important whether he is well read or not. Today the medical literature is replete with information about diet in spite of how important it is in helping cancer patients. If he says you can eat whatever you like – I am sorry, I am not sure if this is the kind of doctor you should go to! I am fully aware that diet in cancer is a big, sore point between medical doctors and alternative medicine practitioners. Suffice for me to quote what two doctors said about diet (below). Think hard about what your doctor tells you about diet and come to your own conclusion. If you are not convinced that he is right, how do you expect him to be able to solve the bigger problem of treating your cancer?
Let us assume that you are a person with a magic touch – what you say is granted – What would you do if you see more and more cancer people getting cancer every day? (Note: in USA alone, more than 1,500 people will die of cancer per day).
The experts surrounding you would probably advise you (assuming you don’t know how to think for yourself): Build more cancer hospitals! Trains more oncologists! Make chemo-drugs cheaper and easily available to all those who need them! Bravo problem solved. QED (Quiet Easily Done was what my mathematics teacher said we should write at the end of our assignment after solving a problem).
A brilliant suggestion indeed! So you think, but you can be dead wrong!
Let me share with you these e-mails. And I get to receive such e-mails or hear such horror stories all too often.
Dear Dr Chris Teo,
I came to know about you after reading Betty Khoo-Kingsley’s book on Cancer Cured and Prevented Naturally. I am amazed on your method of treatment and I believed you may be able to help my husband who is a cancer patient.
My husband was diagnosed with nose cancer in August 2010. He did radiation and it went into remission. The cancer recurred the following year after a year’s break. He did three cycles of chemotherapy but it did not work and he underwent surgery in November, 2011.
In May 2012, PET scan showed a recurrence. He did another three cycles of chemotherapy and the chemotherapy failed again.
He had no choice but to do a surgery on his nose again in July 2012. A PET scan done three months after the surgery showed recurrence of cancer again. He was put on oral chemo but the latest PET scan in November 2012 showed the cancer cell had gone into his cervical spine. He is not on any medication now.
I am truly desperate. Thanking you in advance. Warmest regards. God bless.
This is another e-mail, received on 30 December 2012.
Hello Chris,
My father was diagnosed with 4th stage cancer two years ago, when the doctor found a 13 cm tumor around his kidney. The tumor and the kidney were removed by surgery. He has been taking Sutent for the past two years under the treatment and supervision of an oncologist at Hospital KL.
About a month ago, he had fluid in his lungs and was hospitalized. A CT scan showed that the cancer had spread to his lung, bones, lymph nodes, liver and pelvis. The oncologist said Sutent is not working anymore and that they do not recommend taking another stronger medicine as his body is very weak now. So the doctor told him to go home and treat the fluid in lungs first and will not give any medication for the cancer.
I came across your centre with testimonials and would like to seek your consultation on my father’s condition. As my father is a stroke patient together with his lung condition, it may be quite difficult to put him in the car and drive to Penang for consultation. We live in Melaka.
Actually providing facilities – research money, hospitals, more oncologists, more drugs, etc. has proven to be a big flop when the whole concept of treatment is a basically flawed!
That was what President Nixon of the United States of American was trying to do when he declared war on cancer on 23 December 1971. He promised victory within five years. Money was poured into cancer research by the billions – after all American was said to be the first and only nation to have landed a man on the moon. So what is the big deal with conquering cancer? But for many decades the Americans and the world have been misled – even up to this day.
Read what Dr. Margaret Cuomo, has got to say in her book (below):
About The Author: Dr. Margaret Cuomo is a board-certified radiologist and an attending physician in diagnostic radiology at North Shore University Hospital in Manhasset, N.Y. for many years. She specializes in body imaging, involving CT, Ultrasound, MRI and interventional procedures. Much of her practice was dedicated to the diagnosis of cancer and AIDS. She is the daughter of former New York Governor Mario Cuomo and Mrs. Matilda Cuomo and sister to current New York Governor Andrew Cuomo and ABC’s Chris Cuomo.
Dr. Cuomo has observed first-hand the issues related to current treatment methods. Recognizing the lack of significant progress in the prevention of cancer, she wrote this book, which reveals how profit, politics, and personal ambition have hindered progress in cancer research and prevention. Dr. Cuomo interviewed 60 experts across the country and pored over hundreds of studies to analyze why we have lost so many lives despite $90 billion in federal funds spent over the last 40 years on cancer research.
What Did She Say?
·Cancer research has failed us. Cancer research has been a $90 billion waste. Our tax dollars aren’t being spent wisely.
Despite decades of promises and a vast amount of funding, the current model has failed.
We no longer expect to cure cancer and now talk mostly of living longer with the disease.
We’re still using the cut, poison and burn approach. Chemotherapy and radiation have side effects, and they can cause secondary cancers.
Our target should be cancer prevention. But the author was deeply disappointed” to learn that out of the $4.5 billion the National Cancer Institute asked Congress for this year, only about $200 million will go to prevent cancer.
Cancer is big business, and companies that manufacture chemo drugs don’t profit from telling people to drink more green tea and cook with turmeric — elements in Cuomo’s cancer-prevention diet.
This year, about 1.6 million new cases of cancer will be diagnosed and more than 1,500 people will die per day. We’ve been asked to accept the disappointing strategy to “manage cancer as a chronic disease.”
We’ve allowed pharmaceutical companies to position cancer drugs that extend life by just weeks and may cost $100,000 for a single course of treatment as breakthroughs.
Where is the bold leadership that will transform our system from treatment to prevention?
The system designed to study, diagnose, and treat cancer in the United States is fatally flawed. We would like to think that we have the tools to detect cancer early enough to cure it and that our treatments are safe and effective. We trust that compassion, not the quest for professional advancement and profits, is the primary driver of the cancer establishment. Sometimes, all of that is true. Too often, it is not.
For years, I have been observing our “cancer culture” and I have become convinced that it is not structured to do what we most need: to determine how to prevent cancer, and then implement our discoveries. Despite decades of promises and a vast amount of funding, the current model of research has failed us. We no longer expect to cure cancer and now talk mostly about living longer with the disease. We are not doing enough to pursue promising new approaches to prevention, and we are not dedicating sufficient energy to applying the strategies that already work.
Everyone who is diagnosed and treated with cancer has a unique story. Yet their journeys are also alike in many ways, with a painful and arduous course of treatment almost guaranteed. Together, we can change that, but only if we can first agree not to be shackled by the status quo.
In 1971, when President Richard Nixon signed the National Cancer Act, America declared a war on cancer, and for more than four decades we have continued to wage that war. Think of it: 40 years battling a disease, with billions of dollars spent to conduct research, build new cancer centers, and develop new drugs and new medical technologies. Still, victory eludes us. In 2012, according to our best estimates, some 1.6 million new cases of cancer will be diagnosed and about 577,000 people will die of the disease.
Why have we settled for a medical system that allows cancer to be recast as a chronic and tolerable disease rather than one we should try to prevent? Why do so many scientists at the nation’s drug companies and universities turn their backs on the possibility of prevention? How can we transform the agenda?
Dozens of conversations with some of the nation’s most accomplished and respected physicians and cancer researchers have confirmed my belief that while we may never be able to cure most cancers once they take hold, we can find ways to prevent cancer altogether, to eradicate it just as we have virtually wiped out devastating diseases like smallpox and polio.
More than 40 years after Nixon launched the war on cancer, we are not much closer to curing the disease. Why? Because finding a cure is the wrong goal.
In his 1971 State of the Union address, President Richard M. Nixon promised Americans that he would begin “an extensive campaign to find a cure for cancer.” He added: “The time has come in America when the same kind of concentrated effort that split the atom and took man to the moon should be turned toward conquering this dread disease.” The idea made perfect sense. We had made so many strides in so many areas of medicine earlier that century, discovering antibiotics to cure infections and vaccines to curb viruses. Surely, ending cancer would be no more difficult.
More than 40 years after the war on cancer was declared, we have spent billions fighting the good fight. The National Cancer Institute has spent some $90 billion on research and treatment during that time. Some 260 nonprofit organizations in the United States have dedicated themselves to cancer. Together, these 260 organizations have budgets that top $2.2 billion.
As a result, we know much more about the disease than we once did, but we are not much closer to curing it. Almost 1.6 million people were diagnosed with cancer in 2011. Meanwhile, the rates of certain cancers are rising. When have Americans ever waged such a long, drawn-out, and costly war, with no end in sight?
When it comes to treating cancer, we seem to be in a holding pattern. We are still relying on surgery, chemotherapy and other anticancer drugs, and radiation, just as we did 40 years ago. “We are stuck in a paradigm of treatment,” says Ronald Herberman, MD, the former director of the University of Pittsburgh Cancer Institute. And our treatments are not working.
With the “war on cancer,” we may have created a framework that allows us to declare a stalemate, with no expectation of ultimate victory. We may have put generals in charge who think we should start talking about living with cancer as the “new normal.” At least that is what the director of the National Cancer Institute seems to be suggesting when he talks about “making cancer a disease you can live with and go to work with.”
Harold Varmus, MD, who has also served as president of Memorial Sloan-Kettering Cancer Center in New York City, one of the world’s great cancer hospitals, goes on to say, “We have many, many patients with lethal cancers who are actually feeling pretty good and are working full time and enjoying their families. As long as their symptoms can be kept under control by radiotherapy and drugs that control symptoms and other modalities, we’re doing right by our patients.”
What happened to ending cancer?
It’s true that … the prevention of cancer will be a formidable goal. But there are many promising avenues to pursue. It is time to commit our resources to more aggressively studying the ways in which diet, exercise, supplements, environmental exposure, and other factors can influence the development of cancer.
We also must get the word out about the prevention strategies we know are effective. As recently as March 2012, public health experts told us that we could prevent more than half the cancers that occur in the United States today if we applied the knowledge we already have.
1. Attention to diet – Your “daily plate” should contain two-thirds whole grains, vegetables and fruits, and one-third lean protein, including poultry and fish. Cruciferous vegetables, including broccoli, cabbage and cauliflower contain cancer-fighting compounds. Green leafy vegetables such as spinach, kale, and collard greens also have anti-carcinogenic activity. Cooked or processed tomatoes, including tomato juice and tomato sauce, contribute lycopene to your diet, which is a powerful antioxidant.
Berries such as strawberries and raspberries contain the cancer-fighting ellagic acid and blueberries are powerful antioxidants. Add the spice tumeric to your meals – which is being studied for its cancer-fighting properties.
Red meat should be eaten sparingly and processed meats should be eliminated from your diet. Avoid added sugar in beverages and avoid processed foods as much as possible. Buy organic products whenever possible. It’s a good investment in your good health.
2. Limit alcohol consumption – Alcohol has been linked to cancer risk. No more than one drink a day for women, or two drinks a day for men.
3. Stop smoking – which causes cancer for the smoker, and the person exposed to second-hand smoke.
4. Vitamin D – Have your doctor check your blood level of vitamin D. 40-60 ng/ml is the level recommended by over 40 vitamin D experts for cancer prevention. If your blood level is below this range, a vitamin D supplement is recommended. Vitamin D can also be found in salmon, sardines, vitamin D-fortified milk and orange juice.
5. Exercise daily – Exercise is good for your mind and body. Overweight and obesity are known risk factors for cancer, as well as heart disease and diabetes. Keep physcially fit, and maintain a healthy weight.
Include physical activity in your daily life – climb stairs instead of taking the elevator, or walk a few blocks rather than taking a subway or driving. Be a good role model for children – take frequent breaks from your computer – pace while on the phone – do jumping jacks – all of this can be done in your home or office.
6. Read labels on your consumer products and food packaging. If plastic bottles containing water or other beverages, or food containers, contain the number 3, 6, or 7 within a small triangle imprinted on the bottle or package, it contains BPA – a weak estrogen classified as an “endocrine disruptor,” that has been linked to breast, prostate, and ovarian cancers.
7. Read the labels on your cosmetics, body washes, shampoos, toothpaste, and other personal care products , and do not purchase any that contain harmful chemicals such as parabens, pthalates, and triclosans. Good news: In August, 2012, Johnson and Johnson becamse the first consumer product company to commit to removing a variety of chemicals, including the known carcinogen, formaldehyde, from its consumer products (including its subsidiaries Neutrogena, Clean and Clear and Aveeno) by 2015. Hopefully, other major consumer product and cosmetic companies will step forward to follow this important initiative to protect the public’s health.
(Note: This general advice on diet is for those who are still healthy and are not cancer victims yet. For cancer patients your diet will be much more restricted. No, cancer patients just cannot eat what you like. No, what you eat has everything to do whether your cancer is going to recur, spread or healed).
Related Article: Chemotherapy SPREADS and MAKES Cancer More AGGRESSIVE
Tag (not real name) was a 59-year-old man from Indonesia. In April 2011, he had coughs with itchy throat. He went to see his doctors and was give medication but these did not help. In August 2011, he came to Penang for further consultation. A CT scan on 22 August 2011 showed an irregular mass (6.6 x 8.0 cm) in the upper left lung extending to the pulmonary hilum with left hilar and mediastinal adenopathy. He also complained of pain in the left pelvis. MRI done on 6 September 2011 showed lesion at the body of C6, body and left pedicle of the L5 vertebra. This was probably metastatic in nature. The doctor said Tag had a Stage 4 cancer.
Subsequently Tag underwent 5 sessions of radiation treatment to his neck area. He also received Zometa injection and the oral drug, Tarceva. But later EGFR testing showed no mutation so Tarceva was discontinued. Tag underwent chemotherapy with Alimta (Pemetrexed ) plus cisplatin.
Tag was told that chemotherapy would not be able to cure him but would prolong his life. He was told he had 6 months to live.
After radiation and chemotherapy Tag seldom cough and the pain in the cervical and lumbar vertebrae nearly disappeared.
Re-examination of his chest CT scan showed his lung tumour had increased in size. Tag went to China for further treatment in October 2011. In China Tag underwent a biopsy again. The cancer was again confirmed as a poorly differentiated adenocarcinoma. Tag underwent the following treatments in China:
Microvessel interventional chemotherapy using Alimta + cisplatin and nano material.
Cryotherapy under CT guidance.
Iodin-125 seed implantation under ultrasound guidance – 10 seeds were implanted in the lymph nodes.
All done, the treatment in China consisted of 5 cycles of chemotherapy, 2 times of cryotherapy and one Iodine seed implantation. The treatment was spread over a few visits, each lasting 1, 3 or 6 weeks.
In March 2012, Tag returned to Indonesia and continued to receive chemotherapy with Alimta at the local hospital.
In August 2012 Tag returned to China again. After receiving one cycle of chemotherapy his condition “dropped” (worsened). He was asked to go home to Indonesia.
Not satisfied, Tag came to Penang again – to be hospitalized in the same hospital that he had received his first treatment. His main concern was his elevated leucocytes count. He was rather obsessed with this high number. He was only given antibiotics infusion because he refused anymore chemo-drugs. In spite of the antibiotics Tag’s leucocytes count remain stubbornly high.
In the meantime while in the hospital, Tag’s wife came to CA Care and asked for our opinion. The following are the images of his CT and PET scans.
Based on his medical history and failed medical treatment, I told Tag’s wife to learn how to accept and face reality. There would be no cure. And for him to come to Penang and check into a hospital trying to reduce his leucocytes count was surely mind boggling! He was barking at the wrong tree! Perhaps this is what Professor Jane Plant meant when she wrote, Conventional cancer treatment can process patients to the extent that they no longer understand what is really being done to them. They have lost the ability to think rationally! They come wanting to only hear that they can be cured.
Tag’s wife told me that after a few days on antibiotics infusion, the doctor planned to do a PET scan. I objected to this idea. What is the whole rationale of doing scan over and over again? Know that all these procedures are not good for cancer patients. Do it only if it is absolutely necessary. Just two months ago, you did a CT scan. Now you want to do it again. What do you expect to see and get?
I advised her to bring Tag home as soon as convenient. And if he was agreeable to take herbs, then he can start on our therapy while at home. If he were to stay in Penang, he would have problems cooking, preparing the herbs, etc. It would do him a lot of good to stay home in a familiar environment.
Unfortunately, the next day my wife received a SMS informing us the Tag would want to go ahead and do the PET scan!
A few days later, Tag and his wife came to our centre after being discharged from the hospital. No, his stay in the hospital receiving the antibiotic infusion did not do any good at all. Then Tag complained that his arm was painful after the PET scan and asked if I have any herbs for this. My answer, Go back to your doctor and ask him to “repair” you.
After some days in Penang, Tag and his wife went home to Indonesia with a supply of herbs.
Sometime later, I received an email from his son informing that Tag had gone into a hospital in Jakarta. He still complained that his leucocytes count was high! After a few days, his son wrote to say that Tag did another PET scan and this time he was concerned with the infected lymph nodes in his neck.
On 14 October 2012, I received an email from a medical doctor who is actually Tag’s relative. This is what the lady doctor wrote:
Hi Prof, I had sent you an email last week, did you receive it? Prof, last couple of weeks there was my family member with lung cancer who came to Penang..Now he is in hospital in Jakarta. There is fluid in his lung, The main tumor in his lung grew bigger and so he experienced dyspnea (breathlessness). Doctor wanted to do radiation to the main tumor because it is pressing his airway. I want to ask, can we give him Ascites tea? What do you think of radiation? He keeps drinking your tea. What about the radiation, should he do it? Thank you for your help. Best regards
Reply: Hello B. Sorry for taking so long to write you. I have been busy with so many patients needing my attention. Okay about your relative. I am afraid it is difficult for me to say anything or help. He did not follow my advice. Even when he was in Penang he was in the hospital trying to make his leucocytes count lower!!! I told him you are doing the wrong thing in the wrong hospital. When the doctor wanted to do PET scan his wife SMSed my wife. I told him earlier not to do the PET scan.but the next day he did the PET scan! After he went home to Jakarta his son wrote that he had another PET scan!!!
I really don’t know. Since he is in the hospital, let the doctors take care of him. He is NOT like you …you followed what I said. He did not. Well, that is the way it is. I am not angry but I just give up. It is better for me to move on and help others who really need me. Take care and I believe you father is doing fine. Regards, Chris
23 October 2012: Prof, thank you for your reply, but unfortunately patient died last week in a hospital. He had been in ICU for 1 week. I have same problem here too. One of my family member — 29-year-old, breast cancer metastised to the bone, liver, brain, pancreas and lungs. She did all that the doctor instructed — TACI, streotactic for her brain, etc. It is very difficult to persuade any person, if she does not believe us …even after she saw my father’s case. I also give up. Let her make her own decision. At least I have given her all the information. My father is in a good shape, he is gaining weight 12 kg, but still on Iressa. Regards, B.
(Note: Why did this lady doctor, B write such an email? The full story of her father’s recovery from advanced lung cancer is found in my latest book below – Chapter 11 Lung-Bone-Brain Cancer: When Doctor and Herbalist Collaborate Miracle Happens.)
2. Difficulty to recognize that doing nothing could be a better option!
The behavior of this patient really puzzled me. He came to ask for our opinion. He wanted to try our herbs, but he would not listen to what we say. There is no reason for such person to come and see us in the first place! Even more so, this man had done all the medical treatments and nothing had helped him. But why go on doing the same thing all over again?
In trying to understand him, I asked, What is your occupation? This is one question I would never my patients, especially during the first visit. To me who you are is not relevant and I don’t want to be bias or influenced by your answer. But in this case I thought by knowing what he is will shed some light about the attitude of the person. His answer: I am an administrator in the government. That explains it all. I told him, Your job is to make people follow rules. If they don’t follow what you say, you give them “hell.” You follow the rules handed down to you without questioning. You can do that with the human beings that you “administer”, but unfortunately cancer in you does not behave according to your wishes or rule. You have cancer in you and you want the leucocytes count to come down – by just decreasing that number does not cure you at all. I told you not to do the PET scan but you did it anyway because the doctor said so! You follow “the authority“ like you do in your job. Unfortunately it does not work when it comes to cancer.
3. Not all patients who come to us find healing!
At our centre is a poster on the wall. It says:
You come to find the best doctor There is none here, because the best doctor is found within you. We too wish to find the best, that is the best patient.For it is with the best patient that we can both find healing together — for you!
Tag came to us after knowing that the father of the lady doctor above recovered from his lung cancer. This man had cancer in 2010, a year earlier than Tag. His cancer is more advanced than Tag’s –having spread from his lung to his brain and bone. Yes, this man is still doing fine as of this writing. Why does he not die likeTag? It is because he chose “to do nothing.” Doing nothing does NOT mean that you go home and wait to die! It means you do not need to follow “the so-called established authority” and follow what they tell you to do. Dr. B’s father refused to “medical authority”. He went for alternative therapy. Unfortunately it did not work out well at first. He went down to the bottom of the pit before he found CA Care. That was when his two daughters flew to see us in Penang asking for help. Daughter B is a medical doctor and we agreed that we should work together and avoid as much invasive and toxic treatments as possible. The patient recovered.
Tag was able to see what happened to Dr. B’s father, who actually is a relative. But Tag wanted to follow his own path – doing things his own way. He followed the well established “rules” because he was “trained” not to question “authority.”
On Mon, Oct 15, 2012 at 11:18 a.m., the patient’s sister, MM, wrote me this email.
Dear Mr. Chris,
I saw your website accidentally this morning. I tried to search about the other ways of giving treatment to cancer patient whom doctor has already given up after giving chemotherapy treatment for 7 times. The first and second chemotherapy were given every 2 weeks. The third was given weekly 3 times and fourth chemotherapy given 2 cycles. The last 2 cycles of 4th chemotherapy showed the CA 125 (CA 19.9) increase … Based on these lab tests, the doctor suggested to stop using the same chemotherapy drug and change to other drugs. This is to be done on 16 October, and stressing that the drug is not for curing but only for prolonging life.
After discussing with family, I plan to go for herbal and found your website. At the same time, we are now staying at XYZ Hospital, Penang. So, I already tried to make an appointment with you this Friday at 3 p.m. and shall bring all medical report of the patient. For your information the patient is my youngest sister.
Reply: If you are in Penang, come and see me tomorrow at 10.30 a.m. Go to www.cacare.org and you see map in there. No need to bring the patient, but bring all medical reports. I don’t think you need to do the chemo tomorrow yet. Wait until you come and see me first.
MM wrote, She is very weak, hard to walk and sleep, her tummy getting bigger of the tumor cancer and liquid inside. Actually I would like to ask your opinion about the need to continue the next chemotherapy which doctor said is not meant to cure only to prolong life. The next chemotherapy is tomorrow on Tuesday.
Reply: I don’t think you need to do the chemo tomorrow yet. Wait until you come and see me first. Chris.
Meaningless Decrease and Increase of Tumour Markers
The initial chemo treatment cause both CA 125 and CA 19.9 to drop drastically. But that did not mean much. After more chemo, these markers started to rise again. And it was at this stage that the oncologist told the patient’s sister that the treatment did not work. She needed to go for more chemo using other drugs. Or she could just go home – and go ahead and take herbs if she would like to do so!
Date
CA 125
CA 19.9
10 August 2012
6,794
90,055
22 August 2012
2,798
49,301
18 September 2012
1,260
14,694
25 September 2012
1,462
21,496
2 October 2012
1,739
25,110
Do You Need Tumour Markers to Tell You That Patient Was Getting Better or Worse?
Medications While In Hospital
Based on the medical bills, MM was given the following medications while in the hospital.
Table 1: Medical drugs given to patient during one and half months in hospital
Short of breath, rapid heart rate, trouble concentrating, easy bruising, unusual bleeding, purple or red pinpoint spots under your skin, fever, chills, body aches, flu symptoms, sores in your mouth and throat, stomach pain, dark urine, clay-colored stools, jaundice, numbness or tingly feeling in hands or feet, hearing or vision problems, low magnesium (confusion, uneven heart rate, jerking muscle movements, muscle weakness or limp feeling, nausea, vomiting, loss of appetite, tired feeling.
Chlorpheniramine
Allergies, itchy, sneezing
Fast or uneven heart rate, mood changes, tremor, seizure (convulsions), easy bruising or bleeding, unusual weakness, short of breath, urinating less than usual or not at all, dizziness, drowsiness, dry mouth, nose, or throat, constipation, blurred vision, feeling nervous or restless.
Controloc
Acid reflux
Most serious: allergies – hives, swelling or closing of air passages and throat. Less serious: flatulence, stomach upsets, diarrhea , insomnia.
Dexamethasone
Anti-inflammatory, immunosuppressant steroid
Acne, dry skin, thinning skin, bruising or discoloration, slow wound healing, increased sweating, headache, dizziness, spinning sensation, nausea, stomach pain, bloating, muscle weakness,vision problems, swelling, rapid weight gain, severe depression, seizure (convulsions), bloody or tarry stools, coughing up blood, low potassium (confusion, uneven heart rate, extreme thirst, increased urination, leg discomfort, muscle weakness or limp feeling), dangerously high blood pressure (severe headache, blurred vision, buzzing in your ears, anxiety, confusion, chest pain, shortness of breath, uneven heartbeats), sleep problems (insomnia).
Diphenoxylate / atropine (Lomotil)
Diarrhea
Stomach pain or bloating, diarrhea (watery or bloody), numbness of hands or feet, depressed mood, confusion, fast heart rate, urinating less than usual or not at all, drowsiness, dizziness, headache, tired or restless feeling, nausea, vomiting, upset stomach, loss of appetite, skin rash, or itching.
Dormicum
Sedative
Gastrointestinal disturbances, changes in libido, skin reactions, anterograde amnesia (selective memory loss), depression, restlessness, agitation, irritability, aggressiveness, delusion, rages, nightmares, hallucinations, abrupt withdrawal of Dormicum may provoke seizures.
DURAGESIC patch
Pain
Slow heart rate, weak or shallow breathing, sighing, severe drowsiness, confusion, extreme fear, unusual thoughts or behavior; feeling like you might pass out, dry mouth, nausea, vomiting, constipation, headache, drowsiness, tired feeling, white patches or sores inside mouth or lips.
Eprex
Anemia, bone marrow to produce red blood cells
Hypertensive crisis, brain problems or seizures, nausea, deep vein thrombosis – this may be fatal, diarrhea, flu or flu-like symptoms including fever, jointpain, musclepain or tenderness, pulmonary embolism – this may be fatal, skin rash, vomiting, heart problems, oedema of the extremities.
Heparinised Saline injection
Anticoagulants, prevent blocking by blood clots
Unexplained nosebleeds, bleeding from gums when brushing teeth, red or dark brown urine, bloody or black stools, rash, itching, hives on the skin, swelling of the face, lips, tongue or other parts of the body, shortness of breath, wheezing or trouble breathing, fever, chills, runny nose, watering eyes, vomiting, nausea, itchy soles of the feet.
Decrease of blood cells, Numbness, tingling or burning of hands and feet, Increased blood pressure (severe headache, blurred vision, buzzing in your ears, anxiety, confusion, chest pain and shortness of breath, uneven heartbeats), Seizure, pale skin and unusual weakness, Fever, chills, body aches and flu symptoms, Joint and muscle pain, swelling, redness, skin color, mild nausea, vomiting, diarrhea or hair loss.
Kytril inj
Vomiting and nausea caused by chemotherapy.
Fast or pounding heartbeats, fever, body aches, flu symptoms, easy bruising or bleeding; unusual weakness, headache, stomach pain or upset, loss of appetite, diarrhea or constipation, dizziness; or
sleep problems (insomnia).LexaproAntidepressantConstipation, Insomnia, Dizziness, dry mouth, headache, nausea, exhaustion, Hallucinations, irregular heartbeat, panic attack, allergic reactions, seizures, stomach pain, deteriorating depression, mood change, irritability, severe insomnia, breath shortening, fatigue.Lignocaine InjectionDisturbances in the heart’s rhythmNausea, drowsiness, mental/mood changes, ringing in the ears, dizziness, vision changes, tremors, numbness, headache, backache, fever, unusually fast or slow pulse, trouble breathing, seizures, chest pain, allergic reactions – rash, itching, swelling, dizziness, trouble breathing.MetoclopramideHeartburn, nauseaTremors or shaking in of arms or legs, uncontrolled muscle movements in face, slow or jerky muscle movements, problems with balance or walking, stiff (rigid) muscles, high fever, sweating, confusion, fast or uneven heartbeats, depressed mood, thoughts of suicide, hallucinations, anxiety, agitation, jittery feeling, trouble staying still, swelling, feeling short of breath, rapid weight gain, jaundice, seizure (convulsions), feeling restless, drowsy, tired, or dizzy, headache, sleep problems (insomnia), nausea, vomiting, diarrhea, urinating more than usual.Morphine Sulfate InjectionPainMost serious: respiratory depression. Dizziness, lightheadedness, drowsiness, upset stomach, vomiting, constipation, stomach pain, rash, difficulty urinating, fainting.NeurontinEpileptic and seizuresDizziness, drowsiness, weakness, tired feeling, nausea, diarrhea, constipation, blurred vision, headache, dry mouth, loss of balance or coordination, increased seizures, fever, swollen glands, body aches, flu symptoms, skin rash, easy bruising or bleeding, severe tingling, numbness, pain, muscle weakness, upper stomach pain, loss of appetite, dark urine, jaundice, chest pain, irregular heart rhythm, feeling short of breath, confusion, nausea and vomiting, swelling, rapid weight gain, urinating less than usual or not at all, new or worsening cough, fever, trouble breathing; or rapid back and forth movement of your eyes.OxycotinPain killerConstipation, nausea, drowsiness, dizziness, itching , vomiting, dry mouth, weakness, sweating, loss of appetite, insomnia or abnormal dreams, fever or chills, abdominal pain (stomach pain), diarrhea , indigestion, or heartburn, nervousness, anxiety , or an unusual pleasant feeling (euphoria), shortness of breath, twitching, hiccups, slow heart rate (bradycardia), difficulty passing urine, low blood pressure (hypotension), slow or irregular breathing, ringing of the ears (tinnitus).OxyNorm (oxycodone)Opioid painkillerItching, nausea, vomiting, dry mouth, headache, sleepiness and drowsiness along with dizziness and euphoria (extreme happiness and feelings of well-being), difficulty passing urine, constipation, upset stomach, loss of appetite, slow body movements or tiredness, insomnia, disorientation, low blood pressure, rapid heartbeat, vision problems, hiccups, shortness of breath, fast or deep breathing, confusion, nervousness and anxiety or hallucinations and hypothermia (a drop below the normal body temperature), facial flushing, rigid muscles and nervousness as well as difficulty swallowing, edema (swelling) of the legs, ankles and feet.PanadolPainAllergic reaction – hives; difficulty breathing; swelling of your face, lips, tongue, or throat, nausea, upper stomach pain, itching, loss of appetite, dark urine, clay-colored stools, jaundice, liver and kidney damage.SpironolactoneFluid retention (edema), low potassium levels in the bloodMild nausea or vomiting, dizziness, headache, gas, stomach pain, numbness or tingly feeling,muscle pain or weakness, slow, fast, or uneven heart rate, feeling drowsy, restless, or light-headed, urinating less than usual or not at all, shallow breathing, tremors, confusion, nausea, upper stomach pain, itching, loss of appetite, dark urine, clay-colored stools, jaundice, severe skin reaction — fever, sore throat, swelling in your face or tongue, burning in your eyes, skin pain, followed by a red or purple skin rash that spreads (especially in the face or upper body) and causes blistering and peeling.StilnoxInsomnia and brain disordersHeadaches, nausea, vomiting, dizziness, anterograde amnesia, hallucinations, delusions, altered thought patterns, difficulty maintaining balance, euphoria and/or dysphoria, impaired judgment and reasoning, when stopped, rebound insomnia may occur.XanaxAnxiety, depressionBlurred vision, headache, memory problems, trouble concentrating, sleep problems (insomnia), swelling in your hands or feet, muscle weakness, lack of balance or coordination, slurred speech, upset stomach, nausea, vomiting, constipation, diarrhea, increased sweating, dry mouth, stuffy nose, depressed mood, thoughts of suicide or hurting self, unusual risk-taking behavior, decreased inhibitions, no fear of danger, confusion, hyperactivity, agitation, hostility, hallucinations, feeling like passing out, urinating less than usual or not at all, chest pain, pounding heartbeats or fluttering in chest, uncontrolled muscle movements, tremor, seizure (convulsions) drowsiness, dizziness, feeling tired or irritable.ZantacUlcers in stomach and intestinesDrowsiness, dizziness, sleep problems (insomnia), nausea, vomiting, stomach pain, diarrhea, constipation, chest pain, fever, feeling short of breath, coughing up green or yellow mucus, easy bruising or bleeding, unusual weakness, fast or slow heart rate, problems with vision, fever, sore throat, and headache with a severe blistering, peeling, and red skin rash.ZofranNausea and vomitingDiarrhea or constipation, weakness or tired feeling, fever, headache, dizziness, drowsiness, blurred vision or temporary vision, short of breath, fainting, fast or pounding heartbeats, slow heart rate, trouble breathing, anxiety, agitation, shivering, feeling like you might pass out, urinating less than usual or not at all.
Let me ask you to ponder critically what Dr. Andrew Weil, graduate of Harvard Medical School and currently Director of Integrative Medicine at University of Arizona, said In Health & Healing:
The average patient in a hospital today is placed on half a dozen drugs simultaneously. How some of these chemicals react with each other is anybody’s guess. Moreover, a significant percentage of drug doses in hospitals involve errors: wrong drug, the wrong patient, the wrong dose, the wrong time …. Adverse drug reactions are the leading variety of iatrogenic illness (iatrogenic illness is caused by the effects of medical treatment by the doctors).
Voltaire penned this magnificent snipe: Physicians pour drugs of which they know little, to cure diseases of which they know less, into humans of which they know nothing.
The excesses of drugging in allopathic medicine are one of its worse sins.
I find allopathic medicine glaringly deficient in theory and philosophy of any sort … they have no clear conception or theory of what disease is, nor any general concept of treatment.
We understand – the doctors in the hospital were trying their best to help the patient. They did what they knew based on what they were taught in medical school. But Dr. Weil – a Harvard trained medical doctor concluded that:I find allopathic medicine glaringly deficient in theory and philosophy of any sort … they have no clear conception or theory of what disease is, nor any general concept of treatment.
Why did he say such a thing against his own profession? Let me venture to explain. Take a critical look at the table of medications above again. MM was given 11 to 19 drugs (either orally or infusion) each day while in the hospital. What do these drugs do while in the body? It is anybody imagination! And what is the purpose of each drug – trying to “repair” the damage caused by another drug?
Table 2. Patient received 19 drugs on chemo-day – 18 September 2012
Table 3. Patient received 18 drugs three days after receiving chemotherapy – 21 September 2012
Table 4: Patient received 11 drugs on an ordinary day – 6 October 2012.
Even on an ordinary day (Table 4), her daily staple was 11 drugs consisted of the following:
Albumin injection.
Three types of pain medication – Durogesic patch, Oxycontin, and Oxynorm.
Two types of anti-depression and anxiety medication – Laxpro and Xanax.
Medication to acid reflex.
Medication to prevent blood clot.
Medication for nausea and vomiting.
Medication for low potassium in blood.
Medication for insomnia or sleeping pill.
Why did she need 11 drugs a day?
Why did she need albumin every day?
Where did the albumin go to after infusion each day?
Ask this question:If you give these medications (11 to 19 types of drugs) a day to any healthy person– what do you think would become of that person? Would he/she not go ko-ko?
Study the various side effects that can be caused by each drug received by the patient.
Let’s take albumin injection for example. She was given this injection almost every day for the past one and a half months. This injection may give rise to various side effects such as allergic reactions – fever and chills, rash, nausea, vomiting, hypotension.
So she has to take medication for nausea and acid reflex, for example, to take care of the side effects of albumin infusion.
But this is not all. There are 10 more drugs that she was taking and all of them have side effects.
For example, she took 3 types of pain killers – Durogesic patch, Oxycontin, and Oxynorm. The possible side effects of these drugs are: Slow heart rate, weak or shallow breathing, severe drowsiness, confusion, extreme fear, unusual thoughts or behavior; feeling like you might pass out, dry mouth, nausea, vomiting, constipation, headache, tired feeling, dizziness, itching , sweating, loss of appetite, insomnia or abnormal dreams, fever or chills, abdominal pain (stomach pain), diarrhea , indigestion, or heartburn, shortness of breath, twitching, difficulty passing urine, low blood pressure (hypotension), slow or irregular breathing, slow body movements or tiredness, disorientation, low blood pressure, rapid heartbeat, vision problems, shortness of, nervousness and anxiety or hallucinations and hypothermia (a drop below the normal body temperature), facial flushing, rigid muscles and nervousness, difficulty swallowing, swelling of the legs, ankles and feet.
Looking at the list, is there any wonder that the patient was asked to take two types of anti-depression and anxiety drugs and one type of sleeping pill? Again, these three drugs – anti-depression / anxiety and sleeping pills, would by themselves bring on more side effects. So the list of side effects grows and grows.
On 18 October 2012, patient’s sister wrote:
Her main issues now:
1. Tummy hardened.
2. Hard to breathe.
3. Area on upper abdominal and gastric pain.
4. Swelling of legs.
5. Some redness of allergic that I observed maybe from the vitamin and milk infusion.
6. Hard to relax and cannot sleep well.
7. Tense.
Is this what Dr. Weil was trying to tell us when he wrote: The excesses of drugging in allopathic medicine are one of is worse sins?To Professor Jane Plant, this sounds like a battle between the disease and the treatments – with the patient as the battle ground!
Dr. Weil also said this: Adverse drug reactions are the leading variety of iatrogenic illness (iatrogenic illness is caused by the effects of medical treatment by the doctors).
The question we would like to ask is: To what extent are the drugs given to patient causing the problem? In other words, are her problems caused by cancer or by the drugs that she was asked to take?
Some important questions to ask are:
What is the aim of all these medications? Just to keep the patient alive?
What are the medications that would improve her health and make her healthy?
Is there hope that she would be able to come out of this staple diet of medicines and become normal and healthy again?
What is the philosophy of the treatment? Often we hear, Your cancer can be treated! Yes, it is possible to treat the patient by giving her medications but where is the cure?
Dr. Weil said it out again loud and clear: I find allopathic medicine glaringly deficient in theory and philosophy of any sort … they have no clear conception or theory of what disease is, nor any general concept of treatment.
(Note: As I was writing this sentence, someone sent me an email with this message: Doctors destroy health.)
As a conclusion, let me be clear. I am not here blaming the doctors. They have done their best in wanting to help and save life but unfortunately they have to operate within their medical system, which unfortunately is still stuck in a quagmire.
This is a tragic story of MS, a single, 41-year-old lady from Jakarta.
In early May 2012, MS felt uncomfortable in her abdomen. She felt something moving inside. She went to see an internist in Jakarta. A blood test showed elevated CA 125 – more than 1400. MS was asked to go and see a gynaecologist. A ultrasound was done and the gynecologist told her to go home and pray. She was told consult an oncologist. MS went to see a doctor who treated her with semi—chemo injection.
I was rather curious and enquired more about this treatment! This treatment was provided by a “retired” medical doctor who sees many patients a day. MS was given a concoction of “semi-chemo’ injection every day for two months. For her diet, MS was allowed to take only broccoli juice, egg white (albumin) – 12 eggs a day (4 eggs, thrice a day), banana and pears. MS felt better for the first month of treatment. But in the second month she felt the food rather boring. Her abdomen became bloated. In short, her condition worsened.
MS and her elder sister (MM) came to a private hospital in Penang for treatment in mid-August 2012. She stayed two weeks in Penang and received two cycles of chemotherapy. She went home to Jakarta but did not get any better.
After three days in Jakarta her condition deteriorated (drop!) She was admitted into a hospital in Jakarta due to low albumin. Her abdomen became bigger in size.
On 28 August 2012 MS and MM came back to Penang again and was admitted into the same private hospital. And she has been in this hospital up to this day – almost one and a half months. While in Penang she received seven cycles of chemotherapy. According to MM, the family had already spent RM 100,000 but the patient was not getting any better – in reality MS’s condition had worsened.
Since the current chemo regimen failed, the oncologist suggested switching to another regimen consisted of Caelyx and Topotecan. She was told that this would not cure her, but could prolong her life by about six to eight months. This information shocked MM and triggered here to try and look for another option. MM told me that after a short prayer that night she went off to sleep. The next morning she went to the internet and searched for kanker ovarium. This was her first attempt to find information for herself. There she found CA Care on the YouTube.
MM came to see us on 16 October 2012. She brought along a stack of medical bills but not much medical reports!
From her medical bills, I get to learn many things about staying in a private hospital.
1. It is not cheap to stay alive
The total cost for a 41-day-stay in a private hospital in Penang is almost RM 86,000. This works out to about an average of RM 2,000 per day.
Daily Cost in Hospital
RM (Ringgit Malaysia)
28 August 2012
3,932.70
29 August 2012
1,568.50
30 August 2012
1,436.20
31 August 2012
1,590.80
1 September 2012
2,065.20
2 September 2012
1,917.50
3 September 2012
2,006.00
4 September 2012
1,355.70
5 September 2012
1,723.90
6 September 2012
1,804.30
7 September 2012
1,609.80
8 September 2012
1,663.00
9 September 2012
1,618.30
10 September 2012
1,859.60
11 September 2012
2,459.80
12 September 2012
1,592.50
13 September 2012
1,220.50
14 September 2012
2,999.70
15 September 2012
1,264.50
16 September 2012
1,531.50
17 September 2012
1,178.00
18 September 2012
4,000.80
19 September 2012
2,389.80
20 September 2012
1,479.50
21 September 2012
4,041.70
22 September 2012
2,055.30
23 September 2012
1,856.60
24 September 2012
3,016.20
25 September 2012
2,826.20
26 September 2012
2,312.20
27 September 2012
3,036.10
28 September 2012
2,642.50
29 September 2012
2,164.60
30 September 2013
2,038.50
1 October 2012
2,108.10
2 October 2012
2,922.70
3 October 2012
2,605.40
4 October 2012
1,418.70
5 October 2012
1,664.80
6 October 2012
1,394.20
7 October 2012
1,014.40
Total cost of 41 days in hospital
85,386.30
Average cost of hospital per day
2,082.59
2. The Most Expensive and Cheapest Seven Days in Hospital
At certain days the cost could be as high as RM 4,000 and the cheapest day is about RM 1,000
The most expensive 7 days in hospital
21 September 2012
4,041.70
18 September 2012
4,000.80
28 August 2012
3,932.70
27 September 2012
3,036.10
24 September 2012
3,016.20
14 September 2012
2,999.70
2 October 2012
2,922.70
The cheapest 7 days in hospital
4 October 2012
1,418.70
6 October 2012
1,394.20
4 September 2012
1,355.70
15 September 2012
1,264.50
13 September 2012
1,220.50
17 September 2012
1,178.00
7 October 2012
1,014.40
3. What Makes A Hospital Stay Expensive?
The cost of a hospital stay consist of: room charge, doctors’ fees, nursing care, laboratory services, medical supplies, medication / pharmacy charges, procedures – dressing or nursing, X-ray and CT scan charges.
Laboratory services
RM (Ringgit Malaysia)
CA 125
85.20
CA 19.9
85.20
Full blood picture
53.20
Liver Function Test
47.20
Creatinine
39.60
Prothrombin time (PT)
47.20
Cancer Treatment Monitoring Profile
220.40
Blood-screening and processing
304.00
Blood transfusion
100.00
Imaging
CT scan
880.00
X-ray Charges
800.00
Professional Services
Doctor attendance fee
80.00
Dietetic for follow up
35.00
Nursing care
60.00
Lodging & Physical Facilities
Lodger
20.00
Room – single
310.00
Regular meal – single room
60.00
Clinical waste
10.00
Ripple mattress
20.00
4. The Week of Chemotherapy in Hospital
The Week of Chemotherapy
18 September 2012
4,000.80
19 September 2012
2,389.80
20 September 2012
1,479.50
21 September 2012
4,041.70
22 September 2012
2,055.30
23 September 2012
1,856.60
24 September 2012
3,016.20
Total cost for the week
18,839.90
On 18 September 2012 MS underwent chemotherapy. The drugs used were Carboplatin and Intaxel (generic Indian paclitaxel). And these are the drugs that matters – trying to “kill” the cancer. Take note that the cost of Carboplatin and Intaxel are only RM 363.30 + RM 363.30. But the total cost for the day in hospital was RM 4,000.80. Just imagine, it would be most wonderful if Carboplatin + Intaxel were not toxic – treating cancer would be cheap and everyone could afford it! But the problem is, chemo drugs are toxic, i.e. poisonous! Because of that a lot of other drugs are needed to support and keep the patient alive! Study the details of the costs and types of drugs used for that day.
Itemised bill of 18 September 2012
After receiving the chemo injection, patients generally suffer side effects. Three days later the situation had probably become severe and the patient needed more support. The total bill for the day shot up to RM 4,041.70. Then three days later, further support was needed and this time the bill came to RM 3,016.20
Itemised bill of 21 September 2012
Itemised bill of 24 September 2012
(For information on what these drugs are for, go to Part 2 of this story)
From the above, I learned that to administer a drug to “kill cancer” which costs only RM 363.30 + RM 363.30, patient had to spend more than RM 18,000 in the form of supporting drugs and services. Again I say, how nice it would have been if that RM363 + RM 363.30-chemo-drugs were not toxic to healthy cells. Then we don’t need all those supporting drugs and don’t have to incur all those additional costs.
Can someone “invent”, synthesize or make a drug for cancer that is entirely safe? Or it is AGAINST their vested interest to look into such a proposition? I am not naïve when I ask these questions. Read the quotations below:
DS is a 54-year-old lady from Singapore. In 2010, she had persistent coughs for about six months. In November 2010, she went to the hospital after having severe headaches and vomiting. She was hospitalised for tests. Subsequent imaging procedures revealed lung cancer that had spread to her bones and brain.
Brain scan on 29 November 2010: Multiple small intra-axial solid and ring enhancing lesions in the brain parenchyma. Findings highly suggestive of brain metastasis.
CT Thorax of 30 November 2010: A 4.8 x 4.6 cm mass is seen in the medial basal segment of the left lower lobe. Few satellite nodules measuring up to 1.2 cm are also seen distally in the left lower lobe. Left hilar lymph nodes are enlarged measuring up to 2.6 x 1.4 cm. Further, mediastinal lymph adenopathy is also seen involving the subcarinal and aorto pulmonary lymph nodes. Small subcentimeter sized pre tracheal lymph nodes are also seen.
Bone scan on 8 December 2010: Abnormal uptake projected over the right scapula /glenoid, suspicious of metastasis. Indeterminate uptake at the L5 vertebra. Mildly increased tracer uptake over the right temporal-mandibular junction. Degenerative changes involving the sternum, knees and feet.
DS was treated with Iressa (150 mg daily from December 2010 to mid-April 2012) and monthly injection of Zometa (for her bones). Iressa was stopped after the drug was found to be no more effective.
Her doctor then prescribed Tarceva. From mid-April 20-12 to June 2012, DS was on Tarceva (75 mg daily, and one 150 mg pill taken every two days). DS still continued receiving Zometa infusion once a month.
Within two weeks on Tarceva she suffered side effects such as: pimples and rashes. The doctor reduced the dosage to half. Her tumour marker – CEA – kept on rising. The lung tumour increased in size, her bone and brain metastases worsened.
Vitamins and Supplements
Barley Green / chorella powder
Vitamin B12 or B-complex
Vitamin C – 500 mg
Calcium 800 mg
IP6 (inosital hexaphosphate) 800 mg
Milk thistle
Glucosamine + Chondrotin
Omega 3 or Krill oil
Curcumin extract
Probiotics plus enzymes
Chia seeds, protein shakes, blueberry concentrate.
CT Thorax of 27 October 2011: Since CT scan of 30 May 2011, a mixed response is seen where the dominant left lower lobe nodule shows increase in size whereas the subcentimeter nodule nodule in the left lower lobe lateral basal segment has virtually resolved.
Bone Scan of 13 April 2012: Scan shows foci of increased tracer uptake at: inferior glenoid region of the right scapula (more intense and extensive); T12 vertebra (new) and L5 vertebra (more extensive). Since 25 May 2011, there is interval progression of bone metastases.
MRI Brain with Contrast of 16 April 2012: There are multiple new areas of pial /cortical as well as parenchymal enhancing lesions, highly suggestive of metastases.
Now, the doctor is suggesting that DS undergo chemotherapy with Alimta + Cisplatin. She refused.
DS decided to stop Tarceva and came to Penang to seek our help. She presented with the following:
Pains in left shoulder (scale 5 out of 10) if carry things.
Chest congested and “tight.”
“Crawling” sensation on back of head and sometimes face.
Internal “ticks or twitches” on face.
Sometimes, feet swollen.
Urination 7 to 8 times during waking hours, once at night.
Persistent non-productive coughs. Sometimes felt like being strangled and this feeling passes after a while. Very strong coughing fits sometimes causes urinary incontinence.
Pain in chest after coughing.
DS was prescribed Capsule A, Lung 1 and 2 tea, Brain 1 tea, Bone Tea, Pain Tea and Cough 10 and Cough 11.
Her AcuGraph reading on 7 September 2012 appeared fairly good compared to other cancer patients. She had imbalances of her LU (lung), SP (spleen), KI (kidney) and GB (gall bladder) meridians. Based on this reading, DS was prescribed A-Lung-2 and A-Kid-2 tea.
Comments
If you have been reading our articles in this website, I am sure you would have come across stories of lung cancer patients who have taken Iressa and /or Tarceva. I think I have said and written enough, just read the stories below:




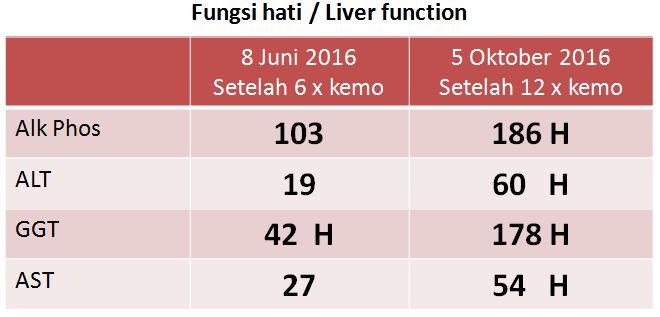








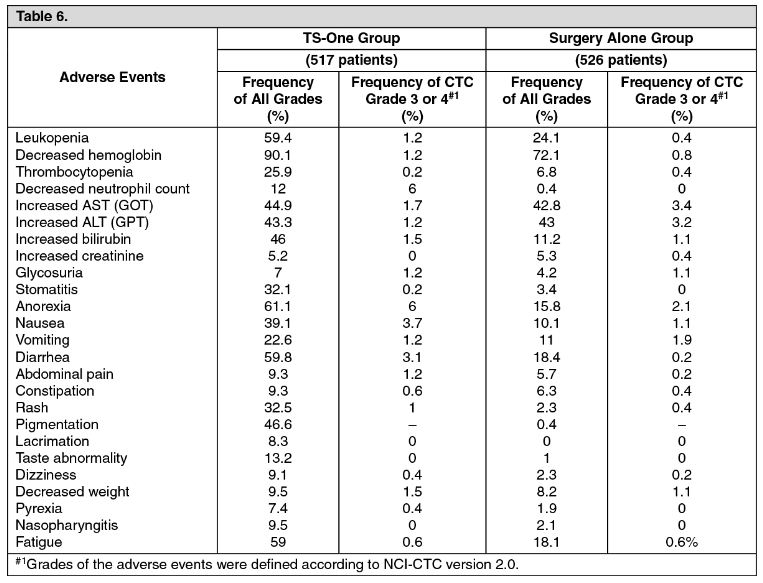


















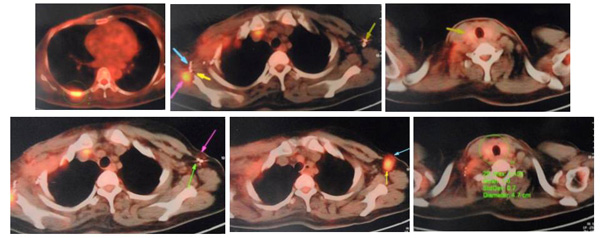


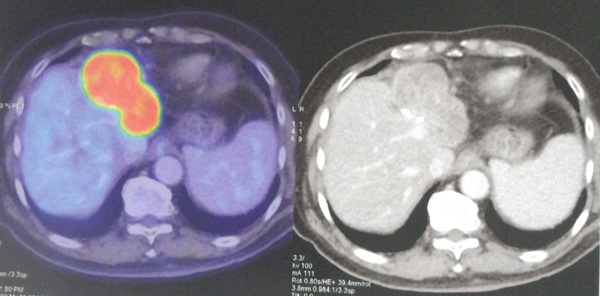






































You must be logged in to post a comment.