
Patients who came to see me with cancerous lumps in their breasts will usually get this standard advice: Get the lump removed, by lumpectomy or mastectomy. No two ways about it. That has always been my position all these years. But in early 2019, I have learned something new! If you have angiosarcoma of the breast, which is indeed a rare cancer, then surgery may not be the answer. Yes, I have learned that it would be a wrong advice if I “push” you to go for surgery for this type of breast cancer.
This is the story of Lily.
Lily is a 31-year-old lady from Sabah. She came to our centre with her mother, in January 2019. Lily found a small lump under the left arm-pit a year ago. Then she found another lump in her left breast. After a scan and biopsy, Lily underwent a lumpectomy. Histopathology report confirmed a low grade angioscarcoma.
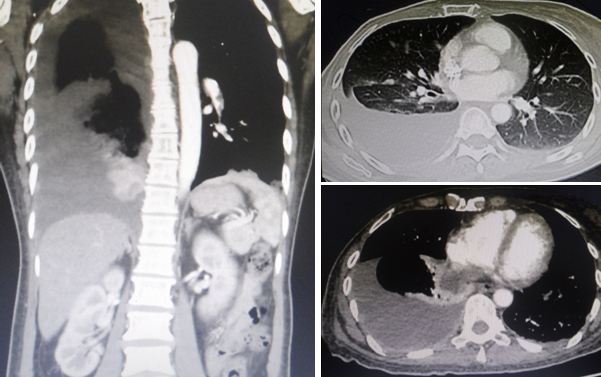
A CT scan was done in November 2018 to look for distant metastases. The cancer had spread.
- There are two masses in the left breast, 2.8 x 3.8 cm and 2.0 x 2.4 cm.
- Lesion in the left pectoralis muscle measuring 2.2 x 3.0 cm.
- Multiple lesions in the chest wall measuring 1.3 x 1.2 cm, 1.4 x 0.9 cm.
- Mass located near the ascending colon and right kidney measuring 2.6 x 3.9 cm.
The doctor suggested surgery to remove the whole left breast. In addition, the surgeon would remove the tumour in the arm, chest wall and stomach. After surgery, Lily was told she may need to undergo chemotherapy.
Atm this moment, Lily was not keen on more surgery and came to seek our help. Listen to our conversation that morning.
Lily: At first the doctor said chemotherapy is not indicated. Later he said it is possible to undergo chemotherapy after the surgery.
Chris: Did you ask if surgery and chemo are going to cure you?
L: No. The treatment may slow down the growth of the cancer or it may even make the cancer more aggressive and spread more widely.
C: Oh, it may slow down the cancer’s growth or it may make the cancer go wild?
L: Yes. And I don’t want to go for the surgery. Even if I do, the result may just be the same.
C: I believe this doctor has not seen too many of this type of cancer before.
L: Correct. The doctor told me so far there are only two such cases in the hospital. Me and another lady, X before me. This doctor performed the surgery on X. Her breast was removed. Then the cancer started to spread to all over the body — including hands and legs. Now, the doctor said he cannot operate on her anymore because there are too many tumours in the body.
C: So what did they want to do with her now?
L: They sent her home to die. The doctor told me that — she is waiting to die.
C: The doctor told you that — just go home and wait to die?
L: Ya. Actually X is a nurse in the hospital.
C: This same doctor is now asking you to go for the same surgery?
L: Ya, that is what it is.
C: He saw the results of what he did to X — then he asked X to go home and die. And now this same doctor is asking you to undergo the same surgery. I can’t understand that.
L: Because of that I am afraid.
C: I understand. I understand you. I cannot promise you anything. But what is the point of undergoing surgery and then you can’t walk, stay at home suffering and waiting to die. No point.
I prescribed Lily some herbal capsules A, C,D and M, in addition to Breast L and M + PLM teas, Lympho + SAP teas and Soft Tissue tea. About two months later, Lily came to our centre again with her monther and father. Listen to our conversation below:
Gist of our conversation that morning.
- My first question to Lily was, How do you feel after taking the herbs. Do they help you in anyway. Unfortunately Lily was not able to answer this question! If the herbs do not help you, why continue to take them? You may want to find another option.
- But it seems that Lily and her parents wanted to continue taking the herbs! But what for?
- Her parents said, What could happen if she does not the herbs? She could be worse off?
- I can understand their logic but I cannot say such a thing because it might appear that I am trying to sell our herbs
- My next question to Lily. After taking the herbs, can you continue to live a normal life?
Do whatever you want to do? Yes, Lily could continue to live a normal life! - Now, what had happened to the nurse who also had breast angiosarcoma and had undergo an operation? She already died within six months as predicted by her doctor.
- I told Lily and her parents. You are on our herbs and two months already. And you are still alive and doing okay. If you can live for another four months, then we “win” in this game! I know all patients who come and seek our help expect me to cure them. I am not God. I cannot cure you.
Since breast angiosarcoma is such a rare cancer, let us turn to the internet and learn more about this cancer.
Ming Yin et al. (https://bmccancer.biomedcentral.com/articles/10.1186/s12885-017-3292-7) wrote:
- Breast sarcomais an extremely rare. The annual incidence of breast sarcomas was 4.48 cases per million women.
- Angiosarcoma is a very aggressive malignant tumor of the vascular endothelium, characterized by rapidly proliferating and extensively infiltrating growth. It carries a poor prognosis.
- Optimal care of breast angiosarcoma is poorly defined because information from previous studies is insufficient and inconsistent.
Katrina N. Glazebrook et al. https://www.ajronline.org/doi/full/10.2214/AJR.07.2909) wrote:
- Primary angiosarcoma of the breast occurs in young women and usually present as palpable masses that may be growing rapidly.
- Secondary angiosarcoma occurs most frequently after breast conservation therapy with radiation therapy. The average latency period is 5–6 years. There are two types of secondary angiosarcoma: lymphedema-associated cutaneous angiosarcoma and postirradiationangiosarcoma.
- Both of these types of angiosarcomas may present with bruiselike skin discoloration.
- Patients with secondary angiosarcomas present with red plaques or nodules or with areas of skin discoloration.
- Surgical resection with mastectomy is the usual treatment for both forms of angiosarcoma.
- With increasing use of breast conservation therapy for breast cancer, reports of post irradiation angiosarcoma have increased.
Suresh Jaywantrao Bhosale et al. https://www.sciencedirect.com/science/article/pii/S2210261213000369) wrote:
- Primary angiosarcoma has a poor prognosis, even after complete resection.
- Surgery is the mainstay of treatment with a limited rolefor chemotherapy and radiotherapy.
- Angiosarcoma usually presents as a palpable mass, but 17% of cases may present with a bluish discolouration or bruising of the overlying skin.
- The frequency of this rare tumouris 0.04% of primary breast tumours and approximately 8% of breast sarcomas.
- Angiosarcoma may present as a painless often discrete palpable mass that grows rapidly.Some patients complain of a painful mass with tenderness. Approximately 2% of patients may present with diffuse enlargement of the breast. However, a bluish red discolouration of the overlying skin may be there.
- Nippleretraction, discharge, or axillary node enlargement are generally absent.
- As angiosarcomas of the breast are very rare, there is no established standard treatment. Mastectomyis the mainstay of treatment. Although some individuals seem to benefit from chemotherapy, it is of minimal benefit for patients with disseminated disease.
Pam Stephan (https://www.verywellhealth.com/angiosarcoma-of-the-breast-430619) wrote:
- To understand breast angiosarcomas, it’s helpful to first distinguish between carcinomas and sarcomas. Most breast cancers that people are familiar with are carcinomas—cancers that begin in epithelial cells, such as those that line the ducts or lobules of the breast. Sarcomas, in contrast, are derived from myoepithelial cells, cells that make up connective tissues such as bones, muscles, and blood and lymphatic vessels. The term “angio” means blood, and angiosarcomas are tumors that begin in blood or lymph vessels. Angiosarcomas may occur anywhere in the body, and the majority of these tumors occur in regions other than the breast.
- Primary angiosarcoma diagnosed in a person who has never had breast cancer may feel like a thickened area of the breast or an ill-defined lump. In some cases, the nearby skin may turn blue or reddish and appear to have a rash or to be bruised.
- Secondary angiosarcomaoften presents with an area of redness or a bluish appearance of the breast. There may also be swelling or a mass in the breast. These lumps, unlike many breast cancers, are often painful.
- Angiosarcomas are less likely to spread to lymph nodes than more common breast cancers, but tend to spread rapidly to distant regions of the body. Sites of metastasis may include the lungs, liver, bones, skin, other breast, brain, or ovaries.
- These tumors have a high rate of recurrence, and may recur locally in the breast or in distant regions of the body.
- Breast angiosarcomas do not often respond to chemotherapy. Radiation does not appear to have any survival benefit for people with primary angiosarcoma, and is associated with poorer survival in people with secondary angiosarcoma.
Omar Ashour and TarannumFasih (http://www.acanceresearch.com/cancer-research/radiation-induced-angiosarcoma-of-the-breast-case-series–review-at-a-single-breast-screening-institution-and-review-of-the-litera.php?aid=9396) wrote:
- Breast conserving surgery with radiotherapy has replaced mastectomy as the standard care for earlystage breast cancerin the last few decades. Angiosarcoma arising in the irradiated breast after breast conserving therapy is being reported in the literature with increasing frequency. As more women undergo breast conserving therapy, the incidence can be expected to increase.
- The risks of developing angiosarcoma of the breast have been attributed to multiple risk factors; this includes trauma, radiation, lymphoedema, and breast implants.
- There is no established standard treatment that is evidence based. Mastectomy however is the mainstay of treatment.
- Although some individuals seem to benefit from chemotherapy, it is of minimal benefit for patients with disseminated disease.





You must be logged in to post a comment.