During this Chinese New Year 2024 – the year of the Dragon! – I had the opportunity to read two books The Red Light Therapy and The Cancer Industry – Crimes, Conspiracy and the Death of My Mother. Both of them were written by Mark Sloan of Ontario, Canada.
Mark’s mother had cervical cancer. She died after surgery, radiotherapy and chemotherapy. Mark wrote:
(This) happened when I was 12 years old. My father called a family meeting in the living room and sat my sister and I down on the couch. We had no idea what he was about to tell us but he looked upset … and I knew at that moment something was terribly wrong.
Dad told us that our mom had cancer.
Doctors found a cancerous lesion on her cervix about the size of a baby fingernail. Dad told us they had detected it early and were going to rush her in for surgery followed by radiotherapy to ensure the cancer wouldn’t return. He assured us that treating her quickly would give her the best chance of survival, and we’ve got the best doctors in Canada working on her.
After surgery and radiotherapy …
Six difficult months passed … back into the hospital for re-assessment. The cancer had spread to her hip area and they wanted to do chemotherapy.
The dramatic decline in her health immediately following chemotherapy was disturbing. Within days of her first treatment, her legs swelled up so badly that she could no longer walk. The poison injected into her veins reduced her jaw muscles to scar tissue so she could barely open her mouth to talk. Chewing food was out of the question so she was reduced to a liquid diet and we began bringing her smoothies.
My mom was able to return home shortly after chemotherapy treatments but her return wasn’t at all glorious like I had imagined. I remember laying in bed late at night and hearing her downstairs crying in excruciating pain. My mother went from looking like a healthy middle-aged woman to something approximating a prisoner of war who had been captured and tortured by the enemy.
The confusion began to set in and then quickly turned to anger: Why was my mother in pain? I thought we had some of the best doctors working on her giving her the best treatments available. She was supposed to get healthy but the treatments have made her worse!!!
A couple months later…
When I got downstairs, Dad was a mess; unable to hold back his tears and struggling to speak.
Dad told us that our mom was gone.
Time to Ponder and Ask Questions
Cancer – surgery, radiotherapy and / or chemotherapy, etc. The patient died. Does this happen often to cancer patients? Unfortunately, the answer could be yes or most likely.
For the following questions, I shall not answer the questions posed but rather quote what Mark Sloan wrote in his books.
2. Can medical treatments cure cancer? This is what Mark wrote (pg. 44) in the Red Light Therapy:
It’s been almost 50 years since the war on cancer has been declared and yet more people are diagnosed and dying of the disease than ever before.
If you give somebody 50 years and around $500 billion dollars in research money to find a cure for cancer and they literally come up with nothing, what do you do? You fire them and find a new approach.
Yes. Many people are being fed with the propaganda that cure is just around the corner! Really?
3. Why can’t they find a cure?
Mark wrote on page 45 of his book:
An industry that makes $126 billion dollars a year will never give us answers, if these answers would mean putting itself out of business.
It is up to us as individuals to understand what cancer is, and the most efficient ways to remedy it.
4. What can be the reality of today’s medical treatments for cancer?
Mark wrote on page 45/46
We’ve all seen at least somebody in our lives undergo surgery, chemotherapy and radiotherapy and then come out far worse than before. I saw it happen to my mother when I was 12 years old. As soon as she received chemotherapy, it was like she got hit by a truck. Instead of recovery, she died a few months later, and every moment from chemotherapy to death was spent in agony.
It is common sense that cutting a sick person with a knife, injecting poison into their bodies, and burning them with ionizing radiation will make their health worse.
It is time to learn from history and take action instead of ignoring it.
5. After much reading, did Mark learn anything?
In his book The Cancer Industry – Crimes, Conspiracy and the Death of My Mother (page 107), this is what he said:
When human being is sick with cancer, they deserve the absolute safest and most effective medicines known.
Yet in this world, cancer patients are routinely rushed into oncology centers where doctors sentence them to death using treatments that make industrial animal slaughterhouse look humane.
My mother didn’t die of cancer. She was murdered-for-profit by an industry that cares more about making money than saving lives.
The monstrous $126 billion dollar cancer industry, hell bent on preserving its profits at any cost, continues its murderous rampage to this day.
The above is Mark’s view. This is what he had learned. You may not agree with him. This is your right.
Let me end by quoting what Dr. Richard Smith said below. Dr. Smith worked at the British Medical Journal for 25 years, serving as editor in chief of the BMJ. Don’t you think he knew “something” that you and I do not know?
Just google this: Death by medical error in US. This is what you get.
Medical errors may account for as many as 251,000 deaths annually in the United States, making medical error the third leading cause of death.
Error rates are significantly higher in the U.S. than in other developed countries such as Canada, Australia, New Zealand, Germany and the United Kingdom (https://pubmed.ncbi.nlm.nih.gov/28186008/).
Medical errors – these are preventable adverse effects resulting from medical care rather than the patient’s condition. We’d like to think they don’t happen.
These issues aren’t new; the first major report on medical errors in the US is from over 2 decades ago. In 1999, To Err is Human from the Institution of Medicine estimated 98,000 deaths due to error. At the time, this would be the 6th leading cause of death in the country.
A study in 2010 found that this number had almost doubled to 180,000 deaths. And by 2013, the estimate ranged from 210,000 to 440,000 deaths per year. This landed medical errors as the 3rd leading cause of death trailing heart disease and cancer.
Light, professor of comparative health policy at Rowan University School of Osteopathic Medicine in Stratford, New Jersey said:
About 2,460 people per week are estimated to die from drugs that were properly prescribed, and that’s based on detailed chart reviews of hospitalized patients.
The estimate, which didn’t include those who died as a result of prescribing errors, overdose and self-medication, would make taking properly prescribed drugs the 4th leading cause of death in the U.S.
FDA approved Vioxx in 1999 as a painkiller. It was being extensively used and prescribed to patients who needed it. Vioxx was later shown to be deadly, causing heart attacks and strokes.
November 2007: Merck announces it will pay $4.85 billion to end thousands of lawsuits over its painkiller Vioxx. The amount … is believed to be the largest drug settlement ever.
To obtain FDA approval, Purdue had to demonstrate that OxyContin was safe and was as effective as other pain drugs on the market.
The FDA approved the application in 1995.
Many doctors began prescribing OxyContin. Doctors wrote 5.4 million prescriptions for the painkiller in 2014. OxyContin became America’s bestselling painkiller, and Purdue reaped $31 billion in revenue.
Rates of addiction and overdose soared alongside the rise in prescriptions.
The U.S. Justice Dept. launched a criminal investigation, and in 2007 the company and 3 top executives pleaded guilty to fraud for downplaying OxyContin’s risk of addiction. Purdue and the executives were ordered to pay $635 million.
The drug is widely blamed for setting off the nation’s prescription opioid epidemic, which has claimed more than 190,000 lives from overdoses involving OxyContin and other painkillers since 1999.
Many years ago, Vioxx was commonly prescribed to cancer patients. Now, this drug has disappeared from the market. What about OxyContin? That too is slowly going off the list although at times, I do know that some patients are still being prescribed with this drug.
But what came as a shock to me is Zantac, a commonly prescribed drug used to prevent and treat heartburn and other symptoms caused by too much acid in the stomach (acid indigestion). Many cancer patients suffer from this problem and they are given Zantac for the problem (even today as I am writing this article).
The chemical name of Zantac is ranitidine hydrochloride.
According to the authors, the British drug company Glaxo said that Zantac does not cause tumours. But the company’s own scientist and independent researchers said this commonly prescribed drug can cause cancer. This fact had been suppressed or kept away from the public for 40 years!
After reading the article I asked myself – It is for real? Or is it just another fake news?
The article went on to say:
This small British company was sometimes called Glaxo University. It conducted important pharmaceutical research that rarely resulted in profitable drugs. Then the scientists at Glaxo Laboratories created a molecule they called ranitidine
This drug is used to heal ulcers and also used to treat heartburn. They developed ranitidine quickly, and the US Food and Drug Administration reviewed it quickly. Glaxo gave it the brand name Zantac.
In 1978 the company was granted a US patent.
For years, Glaxo counted on Zantac for nearly half of its sales and almost as much of its profit. Zantac created reputations and fortunes.
In 2019 the drug was found to be tainted with high levels of a probable carcinogen called NDMA (N-Nitrosodimethylamine).
NDMA, is a yellow liquid that dissolves in water. It doesn’t have an odor or much of a taste. It was first linked to cancer in 1956 and is most toxic to the liver. The poison is created by ranitidine itself. In 2020 the FDA forced it off the market altogether.
From ranitidine’s beginning to its end, Glaxo had been warned by its own scientists and independent researchers about the potential danger.
Over the years, the company backed flawed research — designed to minimize concerns … Glaxo sold a drug that might harm people, tried to discount evidence of that and never gave anyone the slightest warning.
More than 70,000 people who took Zantac or generic versions of it are suing the company in US state courts for selling a potentially contaminated and dangerous drug.
Every public-health agency, from the Environmental Protection Agency to the FDA to the World Health Organization, says NDMA likely causes cancer in humans. But proving that a particular person’s cancerous cells were mutated by a company’s drug is complicated. Glaxo’s decisions suggest it never wanted to consider that possibility. The clues were there. The documents show that Glaxo preferred not to find them.
Lilly stomach cancer drug extends survival vs placebo
The overall survival among patients treated with the Lilly drug in the study was 5.2 months, compared with 3.8 months for those who received a placebo.
Effect of Fruquintinib vs Placebo on Overall Survival in Patients With Previously Treated Metastatic Colorectal Cancer
Median overall survival was significantly prolonged with fruquintinib compared with placebo – 9.3 months vs 6.6 months. (note: prolong survival of 2.7 months).
Median progression-free survival was also significantly increased with fruquintinib – 3.7 months vs 1.8 months (note: extend progression-free survival for 2.9 months).
“Landmark” study shows breast cancer drug Xeloda can extend lives
In one study, Xeloda cut patients’ risk of relapse or death by 30 percent over five years.
74 percent of patients were still alive and recurrence-free, versus 68 percent of women who’d received placebo pill.
Ask this: The difference is only 6% – why do we need to massage the data to become 30%?
In another study – only one group received Xeloda, while women in the other group were given placebo pills. The treatment was given in six or eight three-week “cycles,” with two weeks on the drug, one week off.
Five years later, 89% of Xeloda patients were still alive, compared with just under 84% of placebo patients.
She was cured after 5 years! One year later she died!
MT was 44 years old when she was diagnosed with breast cancer. She underwent a mastectomy followed by 6 cycles of chemotherapy. She also had 30 radiation treatments. After that she took tamoxifen for 5 years.
The promise: The doctor said it was an early stage cancer. MT had a 90% chance of complete cure if she was to undergo all the recommended treatments.
MT believed her doctor and did exactly as she was told. Each year she went back to her doctor for a routine check-up. At every visit she was told that she was fine.
Five years: MT was told to stop taking tamoxifen because she was already cured.
Barely a year later. MT started to have pains in her tail bone and shoulder blade. MT returned to her doctor.
Examination indicated the cancer had spread to her bones.
Why the recurrence? MT asked the oncologist how could this happen – she had done all the treatments required of her. On top of that the oncologist had told her (a year earlier) that she had been cured.
The oncologist’s replied, I do not know why. But don’t blame yourself. It is your fate. Also, the recurrence has nothing to do with what you eat. It is just your fate.
Vincent Coppola, Matt Strelecki and Stan Winokur wrote a book called The Big Casino. It contains 42 articles written by many America’s top cancer doctors. They shared stories that they could not forget about their cancer patients. The title of the book, The Big Casino, suggests that patients seeking treatments in the hospitals in America are not much different than gamblers going to the casinos in Las Vegas or Macau!
Take time to reflect on this. Is going to the hospital for your cancer treatment like going into a casino? Patients and their families put their full trust in their doctors. Cancer treatment these days would cost a lot of money. Some patients would even have to sell their house or land to pay for the hospital bills. Their hope is that the treatment they get in the casino-hospital will make them well again – CURED! That’s the gamble they are taking.
All gamblers know that they cannot win all the time. In fact, you lose more often than you win in this cancer game. Let us examine the reality of what can happen in the casino-hospital.
No Cure for Cancer
Professor Gershom Zajicek, Faculty of Medicine of the Hebrew University of Jerusalem (http://www.what-is-cancer.com) said:
You want to be cured. Unfortunately, most chronic illnesses, e.g. cancer, are essentially incurable. Cure is unrealistic. The only option is to attain a prolonged remission.
Cancer is generally incurable … most statements about cancer do not indicate successful treatment and the vast literature on cancer has to be regarded with scepticism.
Nearer home, a renowned oncologist in Singapore (The Straits Times, Mind Your Body Supplement, Page 22, 29 Nov. 2006) said:
· Oncology is not like other medical specialties where doing well is the norm.
· In oncology, even prolonging a patient’s life for 3 months to a year is considered an achievement.
· Achieving a cure is like striking a jackpot!
· Not all cancers can be cured.
· As doctors, we try our best to cure those who can be cured, to control the disease for those whose lives can be extended, and to comfort those for whom little can be done.
Chemo-drugs Are Not Really Effective
Allen Rose, the worldwide vice-president of Glaxo-SmithKline (Daily Express, 8 Dec. 2003, The Sun, 9 Dec. 2003) said:
Drugs in the market don’t work on everybody.
Drugs for cancer are only effective in 25% of the patients.
Dr. Cynthia Foster (in Stop the Medicine) wrote:
There are plenty of statistics to show that people die sooner if they follow the doctor’s advice and have all the cancer treatments than if they just do nothing.
Doing nothing means not bankrupting themselves with the expensive treatments, not being subjected to medical mistakes and horrible complications. No suffering from dangerous drug toxicity.
Dr. Candace Pert (in Molecules of Emotion) said:
State-of-the-art chemotherapy … was nothing more than different combinations of the same toxic drugs given in different schedules. It continues to kill more people every year, often a slow painful death … by toxic treatments.
Dr. David Agus, a renowned oncologist (in The End of Illness) wrote:
If you come to me for help in treating advanced cancer detected late in the game, your game is likely to be over soon. I say it because it’s the truth. It’s a shame that the technology and innovation in medical research and treatments are so archaic, outdated and dare I say, in some cases barbaric.
Sweet Empty Promise
Within five years, cancer will have been removed from the list of fatal maladies.
The above was the optimistic promise given to U.S. President William Howard Taft in 1910 when he visited Gratwick Laboratory in Buffalo (now Roswell Park Comprehensive Cancer Center). More than a century later, it’s reasonable to ask, What’s taking so long?(https://www.roswellpark.org/cancertalk/201909/cure-cancer-whats-taking-so-long)
On 23 December 1971 (almost 50 years ago) another US President, Richard Nixon tried to fix this cancer problem by signing the National Cancer Act of 1971, launching what was known as the “War on Cancer”. The aim was to find a cure for cancer by increasing research activities and developing more effective treatments for this dreaded disease. After spending billions and billions of dollars on research and decades of hit-or-miss treatment, cancer in general remains a major cause of death up to this day. In short, the war failed.
If all the positive cancer breakthrough headlines are to be believed, then the cure for cancer is right around the corner. But that is a far cry from reality. I think it’s an illusion to imagine that after millions of years of this disease we’ll suddenly find a solution. I don’t think that we’ll ever beat it, but I think that we’ll get it under control so that it becomes chronic but not deadly.
With $200 billion spent and tens of millions of cancer deaths accumulated since 1971, most would say we are losing the war on cancer. Cancer is the top killer worldwide, responsible for 7.4 million or 13% of all deaths annually. In America, cancer will soon overtake heart disease as the top killer, claiming more than half million lives annually.
… don’t except the war to end anytime soon. We’re only really very good at curing mice of cancer.
Overall, during the mid-1970s, the 5-year survival rate among adults for all cancers combined was 50%, today it is about 65%. Admittedly this isn’t that impressive given the amount of resources spent.
Cures for the major killers, such as cancers of the lung, breast and liver, remain elusive primarily because of the unpredictable nature of cancer cells.
Dr. E.H. Ng, Chairman of Medical Advisor of Breast Cancer Foundation, Singapore (in the Foreword of Cheers to Life) rightfully pointed out the reality of today’s cancer world:
Bare facts, statistics and exhortations. Doctors are good at dispensing these. They roll out of their tongues smoothly, falling heavily upon our patients’ ears, impressing upon them the potency of this disease.
After all is said and done, medical science remains remotely far from being able to assure everyone that cancer can be kept at bay or that doctors can cure the afflicted.
Medically, most cancers are best treated with surgery. When surgery is not indicated, cytotoxic drugs are used such as in chemotherapy (now we are entering the age of immunotherapy and targeted therapies). Besides these, patients are also told to undergo radiation therapy. Often 2 or more modalities are used with the hope of getting the best results.
The goal of treatment is to kill as many cancerous cells while reducing damage to normal cells nearby. This is a hard call. Because the toxic treatments may do more harm than good in some patients.
We also need to remember that a cancer in one individual can be very different from the cancer in another individual even though they are the same type of cancer. Within a single type of cancer, such as breast cancer, researchers are now discovering different subtypes that requires to be treated differently.
Perhaps this is the reason why Dr. C. Kent Osborne, director of Breast Cancer at Baylor College of Medicine, Houston said:
Everybody was treated the same way, despite the fact that we know some patients did well no matter what we did and other patients did poorly and died no matter what we did.
Let me share with you some of the “many things” that I learned over the years about cancer and its treatment.
Cancer is the second most lethal disease in the U.S., behind only heart disease.
More than 1.7 million Americans were diagnosed with cancer in 2018, and more than 600,000 died.
Almost four out of ten people will be diagnosed in their lifetime.
Big Business
Cancer has spawned a huge industrial complex involving government agencies, pharmaceutical and biomedical firms, hospitals and clinics, universities, professional societies, nonprofit foundations and media.
The costs of cancer care have surged 40 percent in the last decade, from $125 billion in 2010 to $175 billion in 2020 (projected).
Total research spending since Richard Nixon declared a “war on cancer” in 1971 exceeds a quarter trillion dollars.
Big Bluff
Cancer-industry boosters claim that investments in research, testing and treatment have led to “incredible progress” and millions of “cancer deaths averted,”
Cancer experts and the media often describe new treatments with terms such as “breakthrough,” “game changer,” “miracle,” “cure,” “home run,” “revolutionary,” “transformative,” “life saver,” “groundbreaking” and “marvel.”
There are 1,200 accredited cancer centers in the U.S. They spent $173 million on television and magazine ads directed at the public in 2014.
43 of the 48 top spenders “deceptively promot[ed] atypical patient experiences through the use of powerful testimonials.” A 2014 studyconcluded that cancer centers “frequently promote cancer therapy with emotional appeals that evoke hope and fear while rarely providing information about risks, benefits, costs, or insurance availability.”
No one is winning the war on cancer, Claims of progress are mostly hype, the same rhetoric from the same self-important voices for the past half century.
Azra Raza, an oncologist at Columbia. She has watched too many people die from cancer — her patients and her husband, also a cancer specialist.
New Treatments Yield Small Benefits, Big Costs
Pharmaceutical companies keep bringing new drugs to market. But … 72 new anticancer drugs approved by the FDA between 2004 and 2014 prolonged survival for an average of 2.1 months.
Most cancer drug approvals have not been shown to, or do not, improve clinically relevant end points, including survival and quality of life … the FDA may be approving many costly, toxic drugs that do not improve overall survival.
Costs of cancer treatments have vastly outpaced inflation, and new drugs are estimated to coston average more than $100,000/year.
More than 40 percent of people diagnosed with cancer lose their life savings within 2 years.
Immunotherapy
Immune therapies, which seek to stimulate immune responses to cancer, have generated enormous excitement.
Drugs firms aggressively market immune therapies, and patients are “pushing hard to try them, even when there is little to no evidence the drugs will work for their particular cancer.”
Oncologists Nathan Gay and Vinay Prasad estimated that fewer than 10 percent of cancer patients can benefit from immune therapies, and that is a “best-case scenario”.
Immune therapies trigger severe side effects, and they are also extremely expensive, costing hundreds of thousands of dollars a year.
Subsequent hospital stays and supportive care can drive the total costs to a million dollars or more … If widely prescribed, immune therapies could bankrupt the American health-care system.
Corruption In The Cancer Industry
The American approach (to cancer treatment) fosters corruption.
Many cancer specialists accept payments from firms whose drugs they prescribe. This practice leads us to celebrate marginal drugs as if they were game-changers. It leads experts to ignore or downplay flaws and deficits in cancer clinical trials. It keeps doctors silent about the crushing price of cancer medicines.
Top officials at Sloan Kettering Cancer Center “repeatedly violated policies on financial conflicts of interest, fostering a culture in which profits appeared to take precedence over research and patient care.
GT is a 35-year-old single lady from China. About a year ago (in July 2018) she felt a lump in her left breast. She was asked to do a biopsy and probably followed by an operation. She refused.
GT works as a sales assistant in a health food company. She sells health drinks that are said to boost the immune system. Her boss gave her these “health foods” and she took these for about three months. No, the lump in her breast did not shrink.
GT then turned to TCM – Traditional Chinese Medicine. She consulted a TCM doctor in the hospital.
Chris: The TCM doctor did not ask you to operate and remove the lump in your breast?
Translator: The doctor said, “don’t cut.”
C: Did the TCM doctor say he can cure you?
Translator: Yes. This doctor is quite famous.
C: No, he did not know and he gave wrong advice!
GT was on TCM medications for almost a year. And these did not work for her either.
GT went back to the TCM hospital again. She did a CT scan. The lump in her breast had grown bigger, to 3.8 x 1.8 cm. The cancer had spread to her lungs and bone. Unfortunately, GT did not bring along her CT scan so I am not able to see the extent of her metastasis.
C: What did the doctor say after the CT scan?
T: She was referred to other “bigger” hospital for treatment. But instead of going to the hospital she decided to fly to see you in Penang.
GT presented with breathlessness and severe coughs which make it difficult for her to sleep at night. Otherwise, she looked fine. The lump in the breast is hard and intact, not lacerated.
My advice
If you were to see me earlier when you first discovered the lump, I would have asked you to remove the lump.
This is the safest way for you. If you keep the lump in your breast it will grow bigger and one day it will burst. Do you like your lump to be like the picture below?
In addition to the painful and ugly wound like above, the cancer will spread. It goes to the lymph nodes, lung, bone, liver and finally brain. So you don’t want to take such risk. The longer the cancerous lump is in your breast the higher is the risk that it will spread elsewhere.
You are only 35 years old. You should not take such risk. Also, my experience showed me that breast cancer in young person tend to be aggressive. So, don’t take any chance.
Now, the cancer has already spread to your lungs and bone. I don’t know how extensive it is because you did not bring along your CT scan.
WHAT DO YOU EXPECT ME TO DO for you?
I felt very sad after hearing her story. I was also upset. She was not given the “right” advice. Now her condition had deteriorated with such an “extensive” metastasis. I am afraid her recovery or survival is very slim. And this poor lady flew all the way from China to see me. What can I do? What did she expect me to do for her? That was exactly the question I asked her that morning.
GT’s reply was rather modest. She wanted me to help her with her coughs. I was glad that she did not ask me to cure her! No, I cannot cure her cancer! To help her, may be but not cure.
I spent time talking to GT trying to find out what could be the underlying problems that could have contributed to her breast cancer.
My advice to her that morning:
Physical stress: Her life is too stressful. GT works from 9 a.m. to up till mid-night sometimes. She stays by herself in the city. GT’s boss suggested that she takes a long leave from her job. Yes, I fully agree with that. GT cannot survive for long under such stress.
Emotional stress: What about emotional stress? GT admitted to having problems with her boy friend and she had broke off that relationship. But, she has a lump in her left breast — could it be due to a female rather than a male? GT admitted that a very close female friend had betrayed her. This had upset her very much but GT said that emotional stress has dissipated with time. I said this to GT: Learn to let go — don’t keep any ill feelings in your heart.
Family support: Her parent’s home is about 4-hour-away by bullet train. Life must be hard for GT having to stay alone in a city without any family support. I suggested that GT go home and stay with her parents. She agreed.
Diet: You can imagine what she eats everyday under the above situation. I can guess it cannot be healthy food every day. Unfortunately, the TCM doctor did not give good advice on this important matter. GT was told not to eat sea food and chilly. After much reading and receiving feed backs from our patients, I came to this conclusion: a) Don’t take anything that walks, including eggs and dairy products. b) No sugar c) No oily or fried foods d) Banana is bad for lung problems.
Herbs bitter and awful taste: Our herbal teas are bitter and have awful taste. She needs to brew each of the teas. It takes time and effort. Will she be able to cope with that? I know most patients cannot!
Monitoring: GT needs constant monitoring. After a month, I need to know how she progresses. Herbs need to adjusted. This means, GT may need to come and see me again. Or she needs to take more herbs after she finishes this first round of teas. Staying in China, how can we overcome this problem? Actually this is the problem facing most patients — even for those who live just a few hour’s drive from us. For such people, I never get to see them again after their first visit. What a waste of time and money.
Financial burden: At CA Care, consultation, no matter how long it takes, is free of charge. However, we request patients to pay for the herbs. Since we started CA Care more than two decades ago, the price of our herbal teas never increase in price (in spite of the inflation). We try to be as charitable and helpful as we can. But, we understand that for GT, even flying to Penang from China cost her a lot of money. How nice if there is such a set up like CA Care in her own hometown! For GT, sad to say that I would probably not be able to see her again.
Comments
Not too long ago, I read two news reports about cancer treatment in China that make me feel real sad.
There is a movie, Dying to Survive, which has become a billion-yuan-success after being released in July this year. It is based on a real-life story of Lu Yong, a Chinese textile trader and leukemia patient. He imported less expensive generic drug from India and sold it to his fellow Chinese patients. Lu helped thousands of Chinese patients. Sadly, he was arrested and jailed in 2014 for doing such “illegal” activity.
This movie, Dying to Survive tells the same story in a more dramatic way. It featured an owner of an Indian Miracle Oil Store — Cheng Yong — who found out that the Indian-made generic leukemia drug, Gleevec, was sold at only 500 yuan in India. In China the authentic Gleevec is sold at 40,000 yuan, eighty times more expensive.
Lured by great profit, Cheng smuggled the unlicensed drug to China and sold to Chinese patients at 2,000 yuan. He made good profit and he was also regarded as a hero by many cancer patients who can’t afford the original version of the expensive Gleevec. Looks like he is a real modern day Robin Hood.
Cheng became rich. He then decided to stop the drug smuggling business. He opened a garment factory. However a large number of patients became desperate as they were forced to sell their houses or everything they have to pay for the expensive Gleevec. That prompted Cheng to change his heart, and renew his smuggling business. This time he even sold the drug only at just 500 yuan to save lives. Unfortunately, he was arrested and jailed for five years.
Note: Gleevec is developed by Novartis. In the US patients need to pay up to US$100,000 for the drug a year without government or insurance subsidy.
I got hit by another heart-breaking story. Tang is a 26-year-old doctor in Central China. He was diagnosed with oesophageal cancer, three years after graduating and starting to work. He underwent surgery to remove the tumour but declined further medical treatment.
In China, doctors like Tang, earn an average of 63,000 to 77,000 yuan (US$ 10,000 to 12,200) per year. Tang just could not afford to pay for the expensive, follow up medical treatments.
On day, Tang decided to mysteriously disappear from home. He left behind his bank cards and a letter to his parents saying they would end up having to “spend all your savings and even run into debt just for dragging out my miserable existence for a few years at best. If I let you face the financial burdens and the sorrow of losing a child in your late years, it would be a sin for which I should die a thousand times. I also don’t want to live like a near dead person for the rest of my life. So please forgive me … I’m an unworthy son, and I will pay back your love in my next life.”
After the above two stories, here I was sitting in front of a 35-year-old lady from China who has breast cancer. I felt sad and frustrated. And this propels me to write this article.
What can we learn from these three stories?
The movie, Dying to Survive, has stirred discussion on the accessibility of cancer drugs and treatments in China. The original drug imported from the US are extremely expensive. But there are generic (or copy cat) drug from India which is much, much cheaper. But unfortunately smuggling cheaper drugs into China is illegal.
The movie has highlighted the exorbitant cost of healthcare. Not only in China, it is the same elsewhere in the developing countries. The cost of cancer drugs are being dictated by the “Cancer Establishment” of the developed nations.
The reality about cancer treatment is well understood by Tang, the 26-year-old cancer patient who is himself a medical doctor. After surgery, the next course of action generally is chemotherapy or/and radiotherapy. Based on his note to his parents — these treatments cost a lot of money. But will these treatments cure him? Unfortunately no.
Again in his note Tang explained to his parent the need to “spend all your savings and even run into debt just for dragging out my miserable existence for a few years at best. I also don’t want to live like a near dead person for the rest of my life.”
How many people understand what Tang wrote or understand the reality of the present day, medical cancer treatment? Cure is elusive — at best for some cancer you extend your life for another few months or years. From the experiences over the past two decades, I come to the conclusion that no one on earth can really CURE cancer. Read more here: https://badscienceblindtruth.wordpress.com/2018/09/18/there-is-no-cure-for-cancer/
Second, cancer treatment is expensive.
Third, the side effects of treatments are severe and “killing.” Is it worth it?
But, what bugs me most is this — does this need to happen in China?
I think there is NO reason to. Why can’t the Chinese develop a much cheaper method of healing cancer? Why is there a need to depend on the expensive medical drugs imported from the US or elsewhere? I believe China can come up with a novel healing method of treating cancer if the Chinese doctors, researchers and entrepreneurs are not obsessed with following what the Western world is doing. Don’t follow others, develop your own way!
For more than two decades, I have devoted my life to helping cancer patients by using herbs, diet and lifestyle changes. There is nothing new about this approach. Through the ages, the Chinese sages have been telling us about this.
To the old Chinese, Indian and those who live in east, we are brought up to understand this culture very well. Unfortunately, the younger generations who come after us have failed to learn that heritage. We live like there is no tomorrow and eat “bad, branded food” introduced by the Western world — as a result metabolic diseases like diabetes, heart problem and cancer are on the rise.
Yes, China has the wisdom about promoting healthy life. Yes, there is TCM (Traditional Chinese Medicine) in China but I think the way it is practised needs improvement! The story as related by this 35-year-old breast cancer from China is indeed pathetic. From her story it is clear that she did NOT get the “proper advice” for her breast cancer. This could be the result of ignorance — either of her doctors or herself.
Over the past two decades I have helped thousands of cancer patients without having to use those expensive drugs from the Western world. The irony is that I first learned how to help cancer patients by studying TCM on my own. Since I don’t read Chinese, I had to rely on books written in English by non-Chinese authors. Oh, how I wish I can read Chinese! In spite of his handicap, we at CA Care have done extremely well. There are some 1,000 video clips about our work in YouTube. I have written more than 700 articles about cancer healing which you can read in my blog: CancerCareMalaysia.com
If I can do this in Malaysia, why can’t the Chinese do the same in China. After all, my approach to managing cancer is based on the wisdom of the old Chinese healing masters. I started with a blank mind. Then I started to read and read and read about TCM. I used my “scientific mind” to select what are useful and leave out what I thought are dubious. In other words, I develop my own method. I don’t blindly follow the “standard procedures.”
If Jack Ma can make Alibaba into such a great success story, I am sure there are many others like him who can also do the same with cancer. I think the real problem is to apply the right knowledge. This unfortunately is not easy — yes, there are many doctors, sinseh and researchers in China but are they really THINKERS and INNOVATORS who know how to apply their knowledge correctly? Or are they just following “cookbook” protocols when practising their trade?
One last word about working with cancer. Cancer treatment of today is more about making money and much less about making the patients well. This is what the “Cancer Establishment” of the developed countries is all about. So beware.
Frances M. Visco, the president of the National Breast Cancer Coalition wrote:
Breast cancer patients are tired of “breakthrough” therapies that do not extend life for even a day but do bring millions of dollars to industry, medical institutions and the doctors who care for us … The answer is clear, just stop circling the wagons focusing on financial gain and fame.
This is my basic principle I uphold right from the very beginning when I founded CA Care — to succeed we need dedication and compassion. If we go in there just for money — and only money — we would fail miserably. I am afraid in the Western world, cancer is indeed about money and making more money… that is why it fails so badly.
Let us not forget what the Great Chinese Sage and Physician, Sun Simiao said,
Whenever eminent physicians treat an illness … they must be free of wants and desires, and they must first develop a heart full of great compassion and empathy. They must pledge to devote themselves completely to relieving the suffering of all sentient beings.
I believe there are enough “kind and generous souls” in China or in this part of the world who want to help their fellow citizens in need. Approach cancer treatment as a noble mission to help others in need.
Some random quick facts about cancer problem in China
China has a massive population of 1.37 billion. Cancer is the leading cause of death in China and is a major public health problem.
In China in 2015: estimated 4,292,000 new cancer cases and 2,814,000 cancer deaths. Lung cancer being the most common incident cancer and the leading cause of cancer death. Stomach, esophageal, and liver cancers were also commonly diagnosed and were identified as leading causes of cancer death.
China has an immense cancer problem. The most common types of cancer in males were those of the lung (21.7%), stomach (19.5%), and liver (18.1%). Source: Cancer Biol Med. 2012 Jun; 9(2): 128–132.
In China, cancer rates are exploding … Last year, more than four million people were diagnosed with the disease and nearly three million died from it. Every day, hundreds pour into (hospitals) from all over China. People wait months for a doctor’s appointment, but often it is too late for treatment and the cancer is too advanced.
Breast cancer is the most common cancer among women in China … the cancer has increased at a rate of around 3.5% a year from 2000 to 2013, compared with a drop of 0.4% a yearover the same period in the US.
Breast cancer rates are higher in urban areas of China than in rural areas. And the higher the population density, the higher the rate.
Julie (not real name) is a 54-year-old Indonesia. She was initially diagnosed with TB (tuberculosis) and has been taking TB medication for the past seven months. No, her problems did not go away.
Blood tests showed her CEA was at 39.7 (high) and a CT scan showed a mass in her lung.
The doctor wanted her to do a biopsy and if it is cancerous, Julie would have to undergo chemotherapy. Julie do not want chemotherapy. My question to her, “Why don’t you want to go for chemo?”
Julie had a bitter experience to share.
About 5 years ago (in around February 2013) Julie’s husband was diagnosed with colon cancer. He underwent an operation — performed by one of the best colorectal surgeons in Singapore. He was then sent to a well known Singapore private hospital for chemotherapy. Chemotherapy was started in June and by December Julie’s husband was dead.
After receiving 3 cycles of chemo, he had difficulty walking.
Chris: “Did you still continue with the chemo?”
In spite of the early warning that something had gone wrong, the oncologist still wanted the patient to finish the scheduled six cycles. Julie’s husband eventually completed the six cycles of chemo. Within a few minutes of completing this last cycle — after the “needle” was removed from his arm — he died.
C: “Did you ask the oncologist why your husband died?”
The oncologist said his heart could not stand the toxic drug.
C: Before you started the chemo, did you ever ask the oncologist if chemo can kill?”
The oncologist said the chemo is going to cure him!
C: “In total, how much money did you spend for his treatment?”
About one milyar (one billion) rupiah.
Comments
This is a story of two tragedies. One, Julie had been taking TB drug for the past 7 months because the doctor thought she had TB. She was not getting better.
Julie said every day, throughout the day, she has pain and numbness on the right side of her chest. Once a while blood oozed out from her right ear. She could not sleep at night because of her cough. She had no appetite and felt tired all day long. She became breathless when climbing the stairs.
The doctor was monitoring her progress through X-rays. It was not until May 2018 that a CT scan was done. After seeing the scan, it was not about TB anymore. Could it be lung cancer? Or to be more precise, could it be a metastatic lung cancer?
Why did I say metastatic lung cancer?
Julie told us that in 2011, she had a hysterectomy. Then in 2013, she again had an operation to remove her ovary. I asked Julie if the doctors at the time ever indicated that she had some sort of cancer? Julie did not know. It was indeed unfortunate that such medical history was not taken into account (perhaps they did not even want to know?) when the doctors came to the conclusion that she had TB.
Tragedy number two. Julie was told that she would have to undergo chemotherapy if the biopsy turns out to be positive. No chemo for me — that is Julie’s position. Her husband was killed by that kind of treatment.
Julie specially flew to Penang to seek our help. Yes, we understand her predicament. I have heard many such stories before. If you have colon cancer you don’t have to die within 6 months even if you don’t do any chemo. We have patients living ten years and more, after surgery but without any chemo. So the story of Julie’s husband is pathetic.
I spent almost an hour trying to help her in any way I can. I have also reminded Julie that I cannot cure her — to help yes, but to cure, NO. In a situation like this we can only do our best to heal ourselves. But first and foremost she must be willing to help herself. Are you prepared to take that responsibility?
You don’t have to wait until your partner dies before you believe what these doctors said:
I apologize for writing without the benefit of an introduction, I am writing this email, with hope that I can scheduled an appointment with you, on behalf of my father who has been diagnosed with nose cancer(T2N1).
My father, Aba (not real name), 58 years old, has been diagnosed with nose cancer (T2N1) in February 2017 and was scheduled for 33 sessions of radiotherapy and 6 rounds of chemotherapy (4 hrs of cisplatin IV infusion),with an approximate total cost of SGD$9,700.
He declined the chemotherapy treatment (oncologists here are very persistent, we had to go thru series of ‘debates’) but complied to radiotherapy treatments. We was initially ensured a total recovery. Doctor mentioned that only 30% suffered from mild side effects and seeing my father is young he is confident that my father will be able to spring back to life in seconds.
Little did we knew, radiotherapy is just as bad. He is currently on his 13th session. The tormenting days started as early as day 2. He is unable to eat maybe because of the many big ulcers, sudden chills, fever, nausea/vomiting and scalded skin. He is so weak. And ever since radiotherapy, I noticed he started to develop tight congestive cough at night. As of now, he said he had lost his sense of taste and hearing to his right ear.
On 6/6/17, during a scheduled consultation, we expressed our concern on his deteriorating health, and if there is anything that they can provide to aid him during this time, and they mentioned a few lists of medications in which they don’t recommended. Their only advice is to allow his antibody to fight it off naturally. At the end of the day, we was only prescribe with a tin of Ensure Vanilla powder.
Disappointed with their lack of concerned and couldn’t help feeling betrayed, that was when we finally decided to called it off and stop the radiotherapy treatments.
It has been more than 48 hrs from his last radiotherapy session and he doesn’t seems to be getting any better.
Our family do believe in herbs but we have no knowledge on it. He has been taking rodent tuber and jus rerama (butterfly plant) as supplements for almost a month now. We sincerely hope you are willing to look into my father’s case. My father is eager to take all possible aggressive measures to combat this disease or at least to live peacefully with it.
We understand that this is one of many such requests that come across your desk and greatly appreciate any guidance that you can lend. We live in Singapore and ensure that I have no issues travelling to Penang on behalf of my father for the consultation and also the follow up treatments.
Thank you, in advance, for your help. I look forward to hearing from you at your earliest convenience.
Best of regards.
Reply: Come and see me with all the medical reports and scans … no need to bring your father … only you come ….. fly in the morning … go back in late afternoon.
23 Feb. 2017: MRI – Nasopharynx and Neck — right nasopharyngeal mass (4.8 x 3.9 x 3.0 cm) with extension across midline and into the right parapharyngeal space with right mastoid effusion. Enlarged right lateral retropharyngeal node, 1.4 x 1.2 cm.
23 Feb. 2017: Bone scan — there is no conclusive scan evidence of bone metastasis.
5 April 2017: Diagnosed with T2N1 nasopharyngeal cancer, EBV negative, p16 positive.
30 May 2017: MRI — Since the previous MRI stuy dated 23 Feb. 2017
stable size and extent of the known right nasopharyngeal tumour.
slightly larger right lateral retropharyngeal lymph nodes — 1.5 x 1.2cm fro, 1.4 x 1.1 cm.
larger cystic right level 2 lymph node suspicious for nodal metastasis — 2.2 x 1.5 cm fro, 1.3 x 0.7 cm.
Aba’s daughter (let’s call her Linda) and her husband came to seek our help. We talked for more than an hour. Below are some excerpts of our conversation that morning.
Here are some of the points we discussed.
Do chemo, 100 percent cure, if radiotherapy 80 percent cure
Linda: He was told to go for chemo – 6 times and radiotherapy – 35 times. He declined chemo but went along with radiotherapy.
Chris: Chemo! Can cure or not?
L: The doctor said, 100 percent cure with chemo. The doctor also said if the patient is my father or mother, I would also ask him/her to do the same.
C: So chemo can cure 100 percent. What about radiotherapy?
L: If he did radiotherapy it will be 80 percent cure.
Only 30 percent of patients will suffer mild side effects of radiation
L: The doctor also said that only 30 percent of patients will suffer from mild side effects of radiation.
C: Mild side effects? That’s what the doctor said?
L: The doctor said my father is still young.
C: Did you father know that the doctor said the radiation side effects is very mild?
L: He knew.
C: And after 13 times of radiation, why did he gave up?
L: He had bad mouth ulcers, etc. When to see the doctor and was told no medication to help him. Only let the body’s antibodies (immune system?) help him.
Why are you so against chemotherapy?
C: Chemo would give a 100 percent cure — why don’t you ask your father to go for chemo?
Son-in-law: He wanted to go for it.
L: I quarrelled with the doctor. I have read a lot of stories. Even my uncle — he had one cycle of chemo for his colon cancer and he wanted to die already. Only one shot, and want to die already.
Oncologist pushing my father to go for chemo!
L: The doctor was very, very …
SIL: insisting.
L: When I told the doctor that I don’t want my father to go for chemo, she was like trying to put the blame on me — if my dies, I would be the one responsible for it.
C: The doctor was really pushing you on that? How old is this oncologist?
L: She is a young lady doctor.
SIL: Some young doctors are like that! Very pushy — chemo, chemo, chemo!
L: She said, this is the standard American protocol.
C: (From my experience) Nobody can cure any cancer! There is another young oncologist who told one of our patients. In my professional life as an oncologist, I have not come across a case where a patient dies because of my chemotherapy!
Fellow patient undergoing the same treatment already died!
L: There was another patient who also underwent the same treatment (like my father in the same hospital). Last week my father asked the nurse what had happened to him. The nursed checked and found out that he already died.
Mom with colon cancer. Surgery but refused chemo. Ten years still alive!
L: I read a lot.
C: Before you father got cancer, did you also read?
L: Actually my mother also had cancer — colon cancer. She went for surgery but she refused chemo. It’s now ten years. She never go for any check-up and she is still alive.
7. My take on this case
We cannot change human attitude. So let me tell you honestly — out of ten patients who come and seek our help, only three patients would benefit from our therapy. We cannot help the remaining seven patients because we cannot change their attitudes. We can help the cancer but we cannot help human beings.
You need to take care of your diet. You cannot eat anything you like. So what to eat now? I can’t help people like that! I know many people swear and curse me because I say you cannot eat this and cannot eat that.
SIL: My father is a very stubborn person. He likes to eat — so we have to change him on that.
C: That is the problem. I have no herbs to make him change his attitude, his stubbornness. I can tell you, I give up on such person. No use. My experience is when he gets well, he will not listen to my advice anymore. He eats anything he likes and he dies.
Comments
There are many lessons we can learn from this story.
It pays to read and read, to know more. It is not enough to just go and see an oncologist and believe he/she can take care of you.
Linda read about her father’s cancer treatment. She took note that her uncle almost died after one shot of chemo. Linda’s mother also had cancer. She was told to undergo chemotherapy after her colon cancer surgery. She refused. She is still alive after ten years!
When the oncologist told Aba and his family members that chemo was going to provide a one hundred percent cure of his NPC, Linda was skeptical. You can only be skeptical and dare to question the doctor if you have some basic knowledge of what cancer treatment is all about. Unfortunately, many patients dare not ask. And they don’t read. They swallow everything that is being fed to them!
Experience and wisdom are what you need to look out for when it comes to making life and death decision. Read and ponder the following wise words of Dr. Ruggeiri below.
It is not difficult to understand what Dr. Paul Ruggieri is trying to tell us. Substitute the word surgeon with oncologist and see how the message strikes you! It may sound like this … the first ten years of practice, an oncologist learns how to chemo people …. she is eager to chemo anyone who walks into her office … she is going to show off her stuff …. bla, bla, bla.
So if I have a choice, I would choose an experienced, sympathetic and wise doctor rather than a sweet, young one! (I know it is hard, wishful thinking?).
Radiotherapy provides a 80 percent chance of cure. And only 30 percent of patients suffer side effects. Even that, according to the oncologist, these side effects are mild. Do you believe that?
Obviously this oncologist does not know what it is like to suffer from the treatments she is dishing out to her patients!
Pastor Danny had NPC and underwent chemotherapy and radiation treatments (using the same drugs as recommended for Aba). And he suffered severe side effects.
Suffered severe side effects of radiation – mouth sore, difficulty swallowing, burnt skin, etc.
At the same time, he received two cycles of chemotherapy. The side effects were worse than radiation and he had to be hospitalized. He was unable to sleep, was in pain and became anxious and depressed. He was put on morphine and as a result suffered constipation and hallucination.
The treatment caused much misery. I would rather die – it was miserable and never again!
The oncologist told Linda that chemotherapy can provide a one hundred percent cure! What the oncologist did not tell is that chemotherapy can also come with a heavy toll! Sometimes, chemotherapy kills.
According to Linda, a fellow patient undergoing the same treatment as her father died along the way! Is that not proof enough? Read what these two doctors say.
Last week the newspapers reported that one of Singapore’s most prominent oncologist was suspended for eight months due to professional misconduct. According to this report, Dr. Ang Peng Thiam, a 35-year veteran and medical director of Parkway Cancer Centre, was found guilty of these charges:
That he made false representation to the patient who was suffering from lung cancer that there was a “70 per cent” chance of responding to the treatment he suggested, and
That he failed to offer her surgery as an option.
The patient died six months after seeing this famous oncologist.
The disciplinary tribunal found that Dr Ang “had no reasonable basis” for saying there was a 70 per cent chance of response and felt that he had “wrongly held out false hope” to the patient and her family. He made the claims intentionally even though he knew or ought to have known there was no basis for him to do so.
The judges said doctors were obliged to present the range of viable options and what the pros and cons of each of these were. Patients must get to decide for themselves what treatment they want, the judges added. “It was not Dr Ang’s role to decide, but to inform,” the judges said.
Cancer patients, can you learn anything from the above episode?
SF was diagnosed with cancer. She came to Penang to undergo the necessary treatment. Initially after chemotherpy, the tumours shrunk and the oncologist told her she was cured! But it was not true. The tumours grew back again after one month. SF was asked to go for radiation followed by more chemo. Then she has to go for surgery. That means more medical bills, but the big question remained unanswered: Can the treatments cure her cancer? She wanted a cure. Is cure possible?
C: They asked you for go for 5 sessions of radiation and then chemotherapy. If the tumour shrinks they want to remove the tumour. In addition they want to remove your right kidney and the urinary tube. Okay, let me know – do you have any problem urinating now? If you cannot urinate, I see the need to operate immediately. But you look well and healthy. I also agree that if you get those tumours removed, the cancer will all be gone. But can surgery cure your cancer?
Husband: Right.
C: What if I say that surgery will not cure your cancer?
Consultation without charge
C: At CA Care we have the responsibility to advise patients who come to us. We are committed to give honest evaluation of your situation. We give advice without having an ulterior motive of wanting to sell our therapy. I have made a promise that I shall do my best to read and learn — to be knowledgeable. And I shall share that knowledge with those who need it without charging any fee, no matter how long I talk to them. Most important, I don’t want to mislead patients. But as much as we want to help, please also know that I am not god. I can only do my best.
Go for medical treatments, you die. Follow our CA Care Therapy, you also die. What is your choice?
C: Let me ask you one question, frankly and bluntly. If you go ahead and undergo the medical treatments as suggested by your doctors — i.e. radiation, chemo, surgery, etc. — for sure, you will have more medical bills to settle! And at the end of it all, there is no cure and you die. Are you satisfied with this route?
P: No, I am not happy with that.
C: I understand because even if you do all these treatments, no one can guarantee that you will be cured. There was one lady from Medan. She had breast cancer and underwent surgery, radiotherapy, chemotherapy, etc.. The treatment lasted 3 years but the cancer did not go away. She had to go into the ICU twice after her chemotherapy. She had to sell a piece of land to pay for her medical bills. During one visit to her oncologist she asked, Why is it, after 3 years already, you still cannot cure me? The oncologist replied, Ibu your cancer cannot be cured. This lady decided to give up chemotherapy and came to seek our help. It was too late, even her liver was “gone”! The daughter said, We felt cheated by all these. Yes, I understand. To me, I believe patients should be told well ahead of time the probable outcome of the treatment — even before embarking on any treatment. In this case, she was told the truth only at the very end of the game.
Now, do you understand what I am trying to tell you?
This brings me to another point. You come and see me. Can I cure you? My frank and blunt answer is, No, I cannot cure you. So if you take my herbs and follow my advice — after a month or two you feel healthy and well — can eat, can sleep, can move around but may have some pains here and there. Are you satisfied? Then one day you die. Are you ready to die without undergoing the medical treatments? Tell me, which path do you want to follow.
P: Yes, I am prepared to take this path.
C: Are you sure?
P: Yes.
Husband: Now that you have explained to us clearly, we understand.
C: There is this man who came to see me. His father had lung cancer that had spread to his brain and was semi-conscious in the hospital. The doctors did a biopsy and then gave him 5 sessions of radiation (which cost RM6,000). The man told me, I want my father to live.
I shook my head in despair. I told him, It is better to bring your father home quickly when he is still breathing. It would cost you a lot of money (RM 8,000 instead of RM200) if you have to bring him home in a coffin.
I also told him, There is no need to fight. You cannot win. No chance. Commonsense tells me that 5 sessions of radiation is not going to cure anything! Let us be realistic and honest about this.
Let us understand that all of us will have to die one day. But many say they don’t want to give up easily. They want to fight and fight until death. That is okay with me. Be a fierce fighter. Ibu do you also want to fight until you die? Or are you prepared to say, Okay, I want to live as long as I can without sufferings. When the time comes for me to go, I shall go I don’t want to put up a fight.
Fighting may mean sufferings. Ibu, what is your choice?
P: I want to take your herbs and shall leave everything else to God. If God says I have to go, I shall go.
C: Are you prepared for that? You will not get angry at me if you cannot find a cure?
P: No, our life is in God’s hand. When I came here for medical treatment, I did not understand all these. I really did not understand why the initial treatment did not cure me and the cancer came back. Now, I understand what is going on. Nobody talked to me like this before.
Husband: We came to consult you. Probably God had opened a way for us.
C: People often tell me that God led them to us. May be God did that, but I also need to remind everyone that to get well is also our responsibility. So again, I want you to think carefully before you make this important decision.
P: I have made up my mind. I don’t want any more chemo.
Understanding the CA Care Therapy
Take care of your diet. Those who follow our dietary advice do not die because they cannot eat this or that.
After talking to a patient for 5 minutes, I would know his/her attitude. Cancer is about human being. If you want to get well you have to change — change your lifestyle, your diet, your attitude. I don’t have herbs to make you change. You have to want to change yourself.
Don’t worry so much. Make time for yourself and go for exercise, meditate, etc.
Take the herbs. But remember, these are not magic potion. They don’t cure your cancer.
So, with all of the above — clean mind, clean diet, clean body and with God’s help, I hope you body heals itself.
Tell the tumour inside you, Let’s live together and let’s not give each other any problem. You don’t disturb me and I don’t disturb you. One day, when I die, you –the tumour– will also die along with me. But if you grow too much, I will die earlier and you also die with me. So let us live in peace. If you have this kind of attitude, you will have peace of mind. But if you fight with the tumour, you will suffer. Undergo all those treatments, you suffer. But at the end, you also die.
So, it better that you learn how to live with your cancer. There is no further need to do any more CT scan or PET scan if you don’t want to go for medical treatment. Do all these for what? Nobody can do anything anyway.
One day, if you can’t live a normal life, that means the cancer has come back. I can’t help you anymore. Go to the hospital and ask the doctor to chemo you. Accept reality — if you die, so be it. What else can we do?
So, Ibu you need to understand what can happen if you take this alternative option.
Be grateful
There is this man who had his kidney removed due to cancer. He was asked to undergo follow up chemo. He refused. He did not want to suffer. So he decided to follow our therapy. Now, he is doing fine. He is able to travel the world. He and his wife went to China. Just recently, they went to Portugal. His wife said, He followed your advice. He is happy. No problem at all. He is normal. If he went for chemo, he would surely suffer. So life is good for us. One day, when he has to die, so be it.
So Ibu, I want you to decide carefully.
P: I want to follow your therapy.
C: Are you sure of that? And you would not blame me if things don’t turn out well?
P: No, no, we will not blame you. Please help me right from today.
Comments
This indeed a hard case to handle. If I have a choice, I would not want to take on this case. But I cannot betray our principle that we are here to help the “helpless and the hopeless.” I felt real sorry that SF was let down by her first oncologist. However, I need to remind everyone that not all patients who come to us benefit from our therapy. Only 30 percent would probably benefit, the rest cannot. It is all about you — your belief, your commitment and your willingness to change.
In part 3 of this story, I raised the issue of money. Many people would disagree with me on this. To many of us who benefit from treating those who are dying, the argument is life is valueless. Many would say, if you are going to die why let money stop you from doing what is best! One oncologist told one patient, If you don’t have any more money to pay me, ask your husband to go and rob the bank. Indeed crude.
But look at this problem of money from the viewpoint of the one who has to pay the expensive medical bills. For these common people, raising money to pay the medical bills means selling the house the family is staying in.
I recalled Pak Jam who came to us, looking disoriented and broken. He had to spent RM2,000 per day on his wife who was undergoing chemotherapy for her leukemia in a private hospital. After 2 weeks he said all his savings were gone. He resorted to borrowing from friends and relatives. He came to seek our help because he could not afford treatment anymore. I told him to bring his wife home quickly. Don’t die in Penang. He followed my advice. His wife took the herbs and continued to life for another 3 years! She died because she went for a blood transfusion and they put in the wrong blood type into her!
In this story, I appeared to be against chemo and surgery. No, I am not anti-medical treatments. But at the same time I also know through experience that these treatments can kill or do not cure cancer. This is an undeniable reality. Let me lists some of my experiences.
One lady had a hysterectomy in Jakarta. The surgeon told the patient, You need to go for chemo after this. The patient asked, Can chemo cure me? The surgeon replied, I was practising in Germany for more than 30 years before I came back to Jakarta. I sent ten patients for chemo, ten patients died!
As I was writing this story, one lady form Kuala Lumpur came. She had a big ovarian tumour. She consulted a surgeon in a private hospital who told her. Surgery is not going to cure you. But after surgery, you need to go for chemotherapy. Chemotherapy is not going to cure you either!
A lady from Surabaya was asked to go for chemotherapy for her gallbladder cancer. She refused. Why? She said, My 39-year-old son had lung cancer. He died after undergoing 5 or 6 cycles of chemo. That’s the reason why I don’t want to do chemo.
If you or someone in your family is diagnosed with cancer, you may wish to take time and reflect on the following.
In 2012, there were 37,400 new cancers and in the same year 21,700 died of cancer. That’s a lot of death due to cancer, in spite of them being treated?
The most common cancers in Malaysia are: colon, lung, NPC (nose), lymphoma and prostate for men. For women — breast, colon, cervical, ovarian and lung.
We do not know WHO will get WHAT cancer in our lifetime. But do we have to wait until we get cancer to know what went wrong? That would be too late!
We know that bad diet (e.g. smoking, excessive sugar intake, alcohol, etc.) and unhealthy lifestyle can lead to cancer. Instead of spending so much money to treat cancer why don’t we spend money to learn how to “prevent” or minimize the chances of getting cancer in the first place? Bah, who is interested in that!
The cost of cancer treatments is expensive. You may need to spend all your lifetime savings, pawn your jewelleries or sell your property — land, house, etc., to pay for these treatments.
What if we do nothing?
What ???? … you may die sooner if you undergo all those treatments dished out to you. Doc., you can’t be right on this?
What ??? again ???? … chemotherapy is a waste of money?
Someone in India sent us the link to this article. Thanks for sharing!
A renowned physician Dr B M Hegde has shown how a large number of doctors working in five-star hospitals shortchange patients in order to keep their management happy and enrich their own pockets.
Prof. B. M. Hegde, MD, FRCP, FRCPE, FRCPG, FRCPI, FACC, FAMS. Padma Bhushan Awardee 2010.Editor-in-Chief, The Journal of the Science of Healing Outcomes, Chairman, State Health Society’s Expert Committee, Govt. of Bihar, Patna.Former Prof. Cardiology, The Middlesex Hospital Medical School, University of London, Affiliate Prof. of Human Health, Northern Colorado University, Retd. Vice Chancellor, Manipal University, “Manjunath”Pais Hills, Bejai. MANGALORE-575004. India.
He said:
To a man with a hammer, every problem looks like a nail. Surgeons like to solve medical problems by cutting, just as physicians first seek solutions with drugs. So, if you take your medical problem to a surgeon first, the chances are that you will unnecessarily end up on the operation table. Instead, please go to an ordinary GP first.
1) 40-60% kickbacks for lab tests.
When a doctor (whether family doctor / general physician, consultant or surgeon) prescribes tests – pathology, radiology, X-rays, MRIs etc. – the laboratory conducting those tests gives commissions. In South and Central Mumbai — 40%. In the suburbs north of Bandra — a whopping 60 per cent! He probably earns a lot more in this way than the consulting fees that you pay.
2) 30-40% for referring to consultants, specialists & surgeons.
When your friendly GP refers you to a specialist or surgeon, he gets 30-40%.
3) 30-40% of total hospital charges.
If the GP or consultant recommends hospitalization, he will receive kickback from the private nursing home as a percentage of all charges including ICU, bed, nursing care, surgery.
4) Sink tests. Some tests prescribed by doctors are not needed. They are there to inflate bills and commissions. The pathology lab understands what is unnecessary. These are called “sink tests”; blood, urine, stool samples collected will be thrown.
5) Admitting the patient to “keep him under observation”. People go to cardiologists feeling unwell and anxious. Most of them aren’t really having a heart attack, and cardiologists and family doctors are well aware of this. They admit such safe patients, put them on a saline drip with mild sedation, and send them home after 3-4 days after charging them a fat amount for ICU, bed charges, visiting doctors fees.
6) ICU minus intensive care.
Nursing homes all over the suburbs are run by doctor couples or as one-man-shows. In such places, nurses and ward boys are 10th class drop-outs in ill-fitting uniforms and bare feet. These “nurses” sit at the reception counter, give injections and saline drips, perform ECGs, apply dressings and change bandages, and assist in the operation theatre. At night, they even sit outside the Intensive Care Units; there is no resident doctor. In case of a crisis, the doctor — who usually lives in the same building — will turn up after 20 minutes, after this nurse calls him. Such ICUs admit safe patients to fill up beds. Genuine patients who require emergency care are sent elsewhere to hospitals having a Resident Medical Officer (RMO) round-the-clock.
7) Unnecessary caesarean surgeries and hysterectomies.
Many surgical procedures are done to keep the cash register ringing. Caesarean deliveries and hysterectomy (removal of uterus) are high on the list. While the woman with labour -pains is screaming and panicking, the obstetrician who gently suggests that caesarean is best seems like an angel sent by God! Menopausal women experience bodily changes that make them nervous and gullible. They can be frightened by words like ” cysts” and “fibroids” that are in almost every normal woman’s radiology reports. When a gynaecologist gently suggests womb removal “as a precaution”, most women and their husbands agree without a second’s thought.
8) Cosmetic surgery advertized through newspapers.
Liposuction and plastic surgery are not minor procedures. Some are life-threateningly major. But advertisements make them appear as easy as facials and waxing. The Indian medical council has strict rules against such misrepresentation. But nobody is interested in taking action.
9) Indirect kickbacks from doctors to prestigious hospitals.
To be on the panel of a prestigious hospital, there is give-and-take involved. The hospital expects the doctor to refer many patients for hospital admission. If he fails to send a certain number of patients, he is quietly dumped. And so he likes to admit patients even when there is no need.
10) “Emergency surgery” on dead body.
If a surgeon hurriedly wheels your patient from the Intensive Care Unit to the operation theatre, refuses to let you go inside and see him, and wants your signature on the consent form for “an emergency operation to save his life”, it is likely that your patient is already dead. The “emergency operation” is for inflating the bill; if you agree to it, the surgeon will come out 15 minutes later and report that your patient died on the operation table. And then, when you take delivery of the dead body, you will pay OT charges, anaesthesiologist’s charges, blah-blah-Doctors are humans too. You can’t trust them blindly.
Donald W Light, professor and Joel Lexchin, professor
Rushed approvals result in a poor deal for both patients and cancer research
Unlike most other diseases, cancer instils a special fear and “is treated as an evil, invincible predator, not just a disease.”
The ability of drug companies to charge very high prices, even when most approved cancer drugs provide little gain for patients, drives much of the research, as desperate patients lead some governments and private insurers to pay whatever companies charge.
Officials within the US Food and Drug Administration are enthusiastic about new cancer drugs. Richard Pazdur, who oversees oncology activities for the FDA says that new cancer drugs are so effective that “We don’t have a lot of questions on [these] drugs because they’re slam dunks. It’s not if we’re going to approve them. It’s how fast we’re going to approve them.”
The methodological weaknesses in oncology trials do not support such enthusiasm.
Trials for cancer drugs were 2.8 times more likely not to be randomised, 2.6 times more likely not to use a comparator (single arm), ….
If you don’t have the money to pay for a one day access to this article, try “googling” the subject matter, and with some luck you get a “free ride” and enjoy comments from various sources.
From http://www.sciencedaily.com/releases/2015/05/150507135917.htm: Highly priced cancer drugs get rushed approvals despite poor trial methodology and little effect on the longevity of patients, cautions York University Professor Dr. Joel Lexchin in the School of Health Policy and Management.
“Patients and their doctors should demand that regulators require pharma companies to provide clear evidence of clinical effectiveness of the drugs, resulting from rigorous methodology,” suggests Lexchin. “Drug agencies like the Food and Drug Administration (FDA) and the European Medicine Agency (EMA) don’t actually look at whether people live longer.”
In an article in the British Medical Journal, titled “Why do cancer drugs get such an easy ride?,” Lexchiin and co-author Donald Light, a professor in the School of Osteopathic Medicine, Rowan University in New Jersey, note that accelerated approval and shortened review times also make it a smooth sail for cancer drugs.
Lexchin cites earlier research reviewing solid cancer drugs within 10 years of EMA approval to point out that these drugs improved survival by just over a month.
“Similarly 71 drugs approved by the FDA from 2002 to 2014 for solid tumours have resulted in median gains in progression-free and overall survival of only 2.5 and 2.1 months, respectively,” he says adding, “Also, only 42 per cent met the American Society of Clinical Oncology Cancer Research Committee’s criteria for meaningful results for patients.”
An editorial in the April 23, 2015 British Medical Journal examined the recent accelerated drug approval process for cancer drugs in both the US and Europe. The subtitle was “Rushed approvals result in a poor deal for both patients and cancer research.”
This editorial contains some extremely disturbing statistics and information the authors obtained from reviewing the chemotherapy clinical study literature and other papers over the last 8 to 10 years.
Between 2007 and 2010, … almost 9000 oncology clinical drug trials were compared with trials for other diseases, the former were 2.6 times more likely not to use a comparator and 1.8 time more likely not be blinded (open to bias from the investigators) … this undermine the validity of the outcomes, it also reflect what regulators will allow. (In lay man language this means bad research. And the regulators — FDA, allows that!).
The European Medicine Agency … found that new oncology drugs improved survival by a mean of 1.5 months and a median of 1.2 months.
The 71 drugs approved by the US FDA from 2002 to 2014 for solid tumors have resulted in median gains in progression-free survival of 2.5 months and overall survival of 2.1 months. (Pay thousands of ringgit plus suffer side effects and you live 2.5 months longer? Not cured? As you told about this before you started paying though your nose?).
Post-marketing changes in the package insert (so-called label) were substantially greater for oncology drugs given priority approval as compared to those going through the much longer standard process, which the authors suggest reflects deficiencies in the accelerated review process. (In layman language it means, quicky, sloppy job — a rush to make quick bucks?)
Both the European and US regulators allow companies to test cancer drugs using a surrogate endpoint rather than survival or other more patient-centered outcomes. Tumor size is given as an example of an unreliable endpoint since it is highly variable in predicting overall survival. (In layman language the measure of trial outcome is not reliable. Just making the size of tumor smaller — or tumour shrinkage — may not mean anything. Surely it does not mean the cancer is cured! So, the measure of effectiveness is faulty).
In 2013, two peer-reviewed papers appeared where a total of over 100 oncologists protested against the high prices being charged for cancer drugs when 11 out of 12 approved in 2012 provided only small benefits for patients. (Do you realize that chemo drugs are getting more expensive …the prices of the newer drugs are beyond our imagination. But are they effective? Yes, make you live longer by 2 or 3 months????? But patients want a CURE)
The authors term the approval process an “Easy Ride” and suggest that this serves both patients and research badly.
It can also be argued that the majority of cancer drug development research currently leading to new drug approval is bogged down in merely getting more ineffective drugs approved in the hope that marginal improvements in survival will lead to enhanced profits. (The root of this evil is greed! They go after your cancer or after your money?)
… generally priced so high that the choice is between bankruptcy or declining treatment except for the wealthy.
The results discussed above are consistent with those presented in 2004 by Morgan et al14. Based on reports from Australia between 1992 and 1997, the contribution of curative and adjuvant cytotoxic chemotherapy to 5-year survival in adults was 2.3% whereas in the US it was 2.1%. These results suggest that over this period in these two countries chemotherapy made little contribution to cancer survival. (Yes, they tell you … chemo will give 60% chance, 99% chance, bla, bla …the Australian showed chemo is only 2 or 3% effective).
Furthermore, not much appears to haves changed between 1992 and 2014 from the patient’s perspective. It is important to note that we are talking about cancers that involve solid tumors. (Why change or improve? As it is – the drug companies are happy, hospitals and doctors are happy! And patients believe and trust them!)
BOTTOM LINE: When offered one of the new “wonder” chemotherapeutic drugs, it is important to ascertain the actual expected life extension in order to weigh this against the side effects. Trivial life extensions are sufficient to gain regulatory approval and allow patients to be told the treatment will extend their life. Unless carefully qualified, such an approach appears unethical.
CANCER ! Don’t panic ! Haste is from the Devil ~ Arab saying.
Why do you visit this website? We believe you are seeking information to enable you or your loved ones to make certain decisions about his/her cancer. Our advice is: Read as much as possible. Gather information from different sources. Cast your net wider and read what others from different disciplines have to say about the same subject. Get out of the box and view your problem in a different light.
Often, in the face of fear, hopelessness and panic we forget to use our commonsense. Calm down. A decision made in haste or under pressure is never a good decision. Remember, you don’t get cancer just only yesterday.
When we go to the hospital, we go with full faith and trust. We believe that the doctors have our best interests in their hearts – after all, medicine is a noble profession! Unfortunately medicine has morphed into something else today!
The treatment of disease is not a science … but a thriving industry ~ Sir James Barr, Vice President, British Medical Association.
Physicians are called to service, to put patients’ good above our own. That’s a very spiritual calling. But with … making medicine a business, we’re … losing that sense of purpose and meaning ~ Christina Puchalski, professor of medicine, George Washington University. Reader’s Digest Sept. 2001.
People go where the money is, and you’d like to believe it’s different in medicine, but it’s really no different in medicine. When you start thinking of oncology as a business, then all these decisions make sense ~ Dr. Robert Geller, oncologist. New York Times, 12 June 2007 by Alex Beresen.
On the morning of 31 May 2014, I woke up to read the following titles in the internet! It is sad. But this is the reality of the medical industry! Please read these …
1. Cancer Ads Focus On Emotion, Not Facts: Are Consumers Being Misled About Treatment Options?
Advertisements released by U.S. cancer centers in magazines and on TV may be delivering the wrong message.
The grueling battle with cancer is one that many people undergo with little knowledge already at-hand. Popular outlets such as TV and magazines may prove unhelpful in that regard … these ads focus more on emotion than on facts.
Consumers gain little information about treatment costs, risks, or even its benefits in concrete, quantitative terms.
If the ads were anything to go by, the data suggests that patients would hope for survival rather than evaluate their chances.
2. Analysis Shows Advertising by Cancer Centers Frequently Evokes Hope and Fear, but Provides Little Information.
Advertisements frequently promoted cancer therapy with emotional appeals that evoked hope and fear, while rarely providing information about risks, benefits, costs, or insurance availability. The researchers suggest that the ads may lead patients to pursue care that is either unnecessary or unsupported by scientific evidence.
Pursuit of unnecessary tests or treatment may … expose patients to avoidable risks and contribute to increasing costs.
3. Nine of 10 cancer center ads use emotional fluff to attract patients, with little mention of success rates, risks or cost.
Cancer centers and hospitals are competing for your business …. Many cancer charities use the same methods to raise money, which I discuss in my most popular video.
In their advertisements to the general public, cancer centers in the US use emotional appeals that evoke hope and fear, and rarely provide information about risks, benefits, costs … The approach may lead to unrealistic expectations and inappropriate treatments, it warns.
Emotional appeals were a cornerstone of most ads …. Most stressed survival or potential for cure rather than comfort, quality of life, or patient-centered care.
5. Study: Cancer ads tug at heartstrings, leave out caveats.
Advertisements for cancer centers are inflated with emotions, but fail to disclose the fine print….
A systematic content analysis of these ads found that the content is sharply directed at a would-be patient’s heartstrings:
85% made emotional appeals to consumers b. 61% used language about hope, extension of life, or a cure c. 52% touted innovative, or advanced technology or treatments d. 30% evoked fear by mentioning death, fear, or loss.
Noticeably missing from most of the TV and magazine ads is information about the risks, scientific-supported benefits and cost:
a. 2% disclosed the risks of the cancer treatment b. 5% mentioned cost of treatment
Emotion-based advertisement is a powerful means of persuasion and potentially harmful to the consumer.
6. Cancer Center Advertisements Focus on Emotional Appeals.
MedicalResearch: What should clinicians and patients take away from your report?
Dr. Schenker: Cancer center advertisements are increasingly common. I think it is important for clinicians and patients to be aware of the focus on survival and potential cure in these advertisements, as well as the use of emotional appeals. I would encourage patients to seek more complete and balanced sources of information – and to talk with a trusted physician – when facing important decisions about their cancer care.
The above comments came about as a result of research conducted by Vater et al and published in the Annals of Internal Medicine, 27 May 2014, What Are Cancer Centers Advertising to the Public?: A Content Analysis.
A total of 102 cancer centers placed 409 unique clinical advertisements in top media markets in 2012. They found out that the:
Advertisements promoted treatments (88%) more often than screening (18%) or supportive services (13%).
Benefits of advertised therapies were described more often than risks (27% vs. 2%) but were rarely quantified (2%).
Few advertisements mentioned coverage or costs (5%).
Emotional appeals were frequent (85%), evoking hope for survival (61%), describing cancer treatment as a fight or battle (41%), and inducing fear (30%).
Nearly one half of advertisements included patient testimonials, which were usually focused on survival, rarely included disclaimers (15%), and never described the results that a typical patient may expect.
In her classic essay, Illness as Metaphor, Susan Sontag suggested that the negative metaphor and myths surrounding cancer increase the suffering of patients.
Vater and colleagues ….found that … benefits of advertised therapies were emphasized more often than risks, and specific data were rarely given.
Appeals were largely emotional rather informational, sometimes seemed to equate treatment with cure and most often focused on survival rather than comfort or quality of life.
The authors suggest that the focus may contribute to unrealistic expectations about treatment benefits among patients with cancer … and may even lead to inappropriate treatments.
Almost every day I have people writing or coming to me asking for help about their cancer. This is my advice, no matter who you go to – medical doctor or alternative practitioner.
If you are asked to undergo any treatment, ask the following questions first (don’t be led by the nose):
a. Can the treatment cure your cancer?
b. If the answer is “Yes”, better think a million times before you take the recommended path! My experience shows there is no such thing as a cure!
c. If you are told you have a 60 percent chance of success, make sure that you understand what this percentage means to you. Know that only 6 out of 10 patient succeed! Success may not mean anything! What is it, cure? Know that that this statistics may not apply to you at all. Six succeeded but how sure that you belong to the 6 and not the 4 who failed?
d. Patients tell me that often they get these answers when they ask about their cancer of cure: Ask God! or We shall try and see. Such answers imply that you are in the game of luck, not science anymore.
e. Another favourite answer is, No cure, but can prolong life. Ask, prolong life for how long? Some drugs only prolong life by a few days, a few weeks or a few months, rarely years!
f. Even if the treatment prolongs life, it comes with a great cost in terms of side effects and money. Decide, if the extra time of being alive (but ended up being a vegetable) is worth it?
g. Ask about the side effects of the treatment. Very often the “bad effects” are toned down! Some don’t want to even tell you about them! It is wise to visit the oncology ward of the hospital and see for yourself (and ask) those who have undergone the treatments. Check about treatment by reading what others say in the internet.
h. Ask about the total cost of the treatment. It is foolish to proceed with the treatment half way and then found later that you don’t have to enough money to complete the journey!








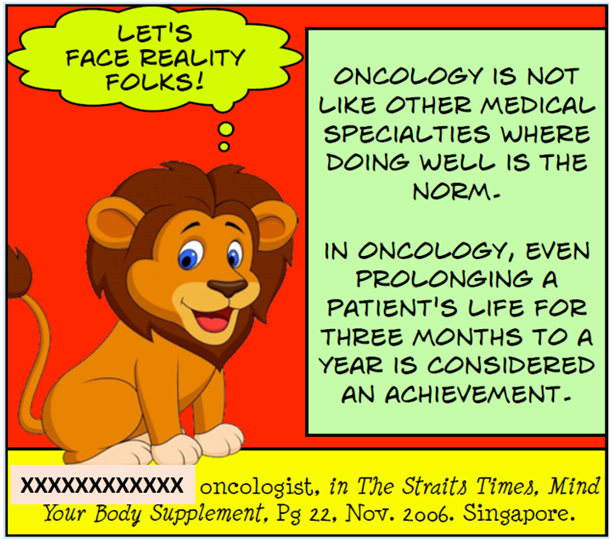







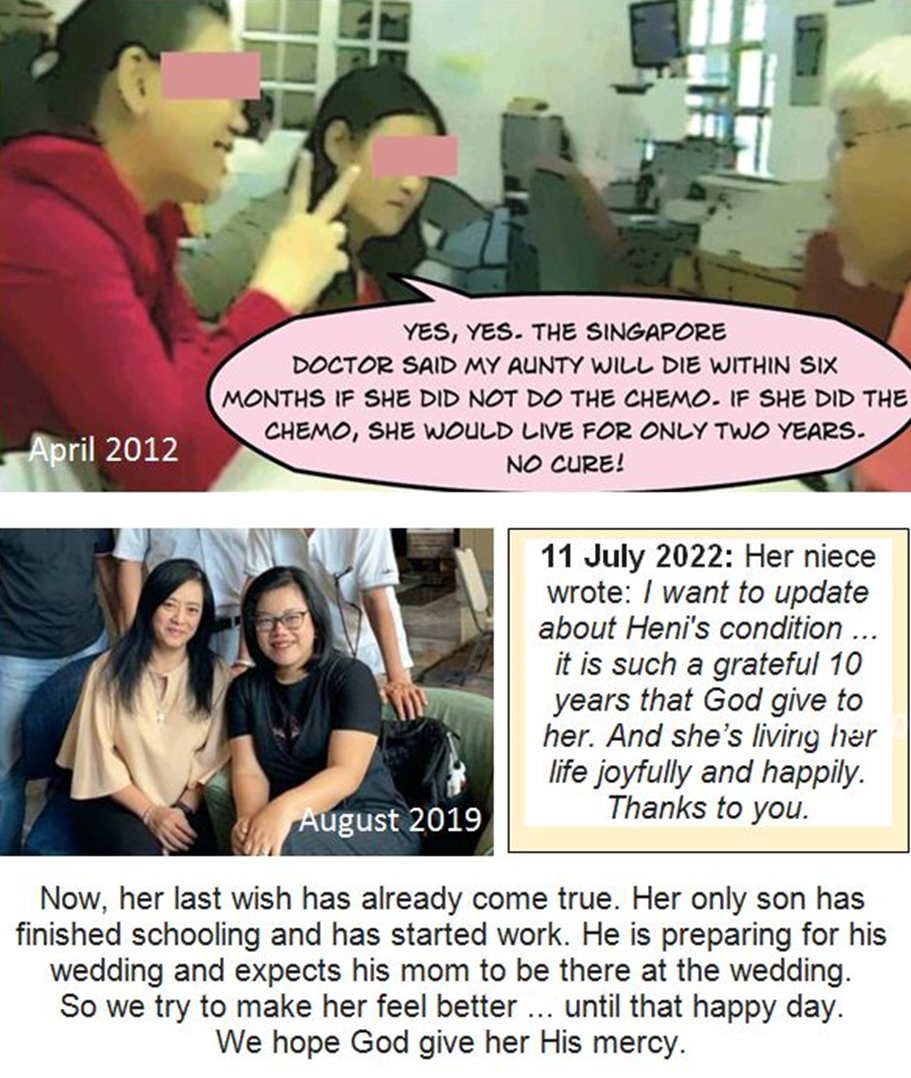












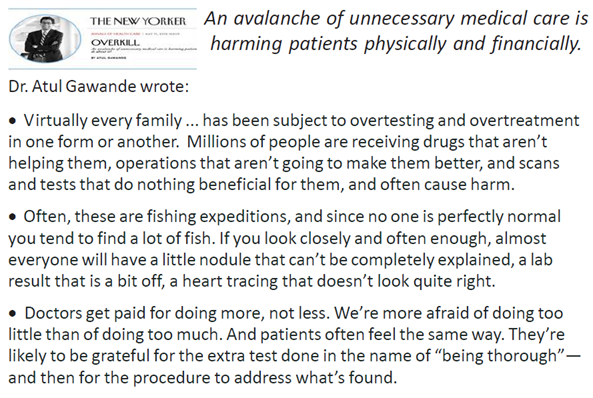







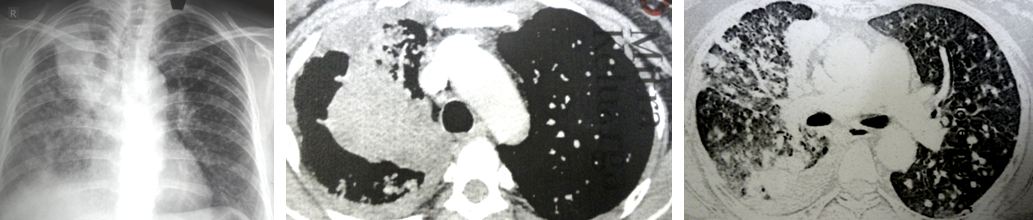






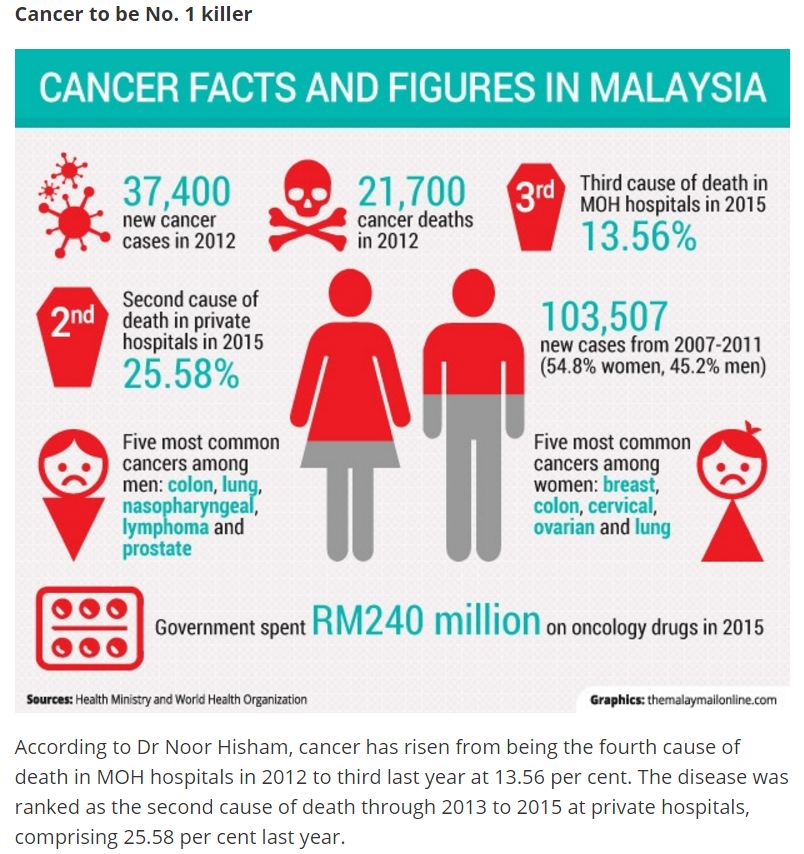

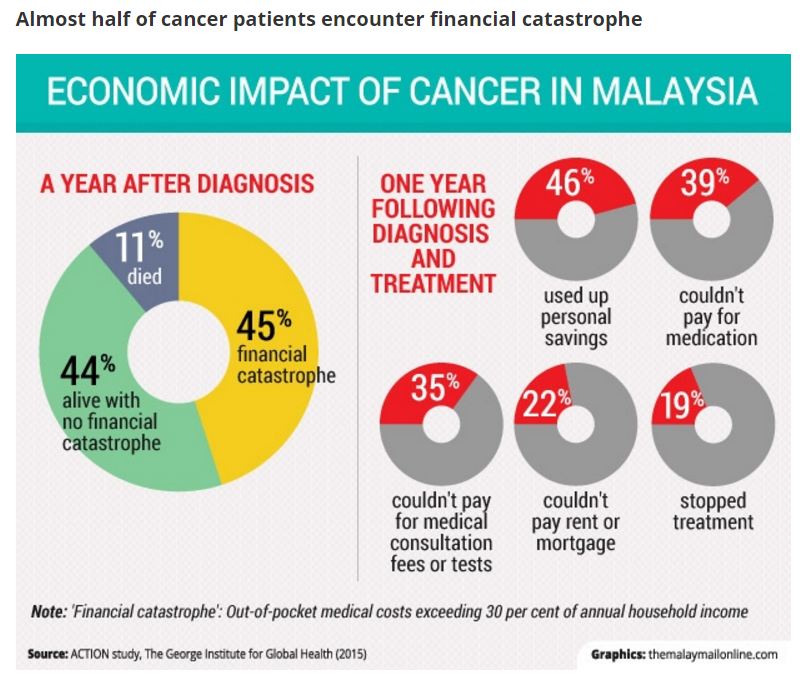











You must be logged in to post a comment.