

This is a normal scenario I often encounter. A patient is diagnosed with cancer. He undergoes surgery immediately, followed by chemotherapy and/or radiotherapy. After completing these treatments, the patient is told to come back for routine check-up. What has to be done, has been done. Probably he thinks, he is cured! But if he knows enough about cancer, deep within, is this scary concern — Can the cancer come back again? Yes, the chances are very high that it would come back.
So, what can you do about it? Nothing much! Wait and see — that probably is the advice given.
The patient goes back for routine check-up once every few months. During this consultation, the doctor may ask a few questions, press here and press there, do a blood test, X-ray, scan, etc. In reality, all these procedures would not help stop the cancer from coming back. On the contrary, it is during one of these procedures that patients could be told that the day of reckoning has arrived! There — another lump! Then more treatments are suggested.
Ask your oncologist what can you do, as a patient, to help yourself so that the chances of recurrence would be minimized? He would probably say, Okay, swallow this pill for prevention or may not be able to give any answer.
Let me share with you this classic example that I often encounter.
HT is a 61-year-old male. His problem started with having blood in his stools. He went to Dr. A in G hospital, and did a colonoscopy. The doctor found many polyps and signs of gastritis. There is a tumour in his transverse colon.
CT scan confirmed colonic neoplasm in the transverse colon with enlarged lymph nodes.
A CT scan done two days later showed two small pulmonary nodules – one in the middle lobe and the other in the left lower lobe, raising the possibility of pulmonary metastasis. There are hypodense lesions in the left adrenal gland which could be metastases.
HT was scheduled to undergo an operation by Dr. A but made a last-minute change to let Dr. B do the surgery instead. The surgeon removed most of the polyps beside performing a hemicolectomy, removing 58.5 cm long segment of this transverse colon.
Histopathology report indicated an invasive moderately differentiated adenocarcinoma. Four out of 28 mesenteric lymph nodes contain metastatic tumour. This is a Stage C2 cancer.
HT then underwent 12 cycles of chemotherapy. The treatment was completed by end of August 2016.
What’s next after chemo? Nothing. But is he cured? Your guess is as good as mine. HT went home to wait — to carry on with his own life! Do what you are doing, eat whatever food you want to eat! But come back for routine check up once every 2 or 3 months.
Dr. Barry Boyd, an oncologist, wrote this:

HT is a typical example of what Dr. Barry Boyd meant — and mind you, what he wrote is what most cancer patients experience most of the time, not only in America but also here. To me, this is one of the main drawback of medical treatment for cancer! Doctor only treats you! But treating does not mean cure. After the completion of the treatment patients are left “in a free fall. This is what I call falling off the cliff.”
HT tolerated the chemo rather well. He only suffered blackening and numbness of the fingers and toes. For that the doctor prescribed Neurobion. He also lost his appetite. His body itched and was given Claritin.
As the chemo treatment progressed, his liver function test values deteriorated. See the 2 tables below. At two months after completion of the chemo, these values deteriorated further which made HT rather worried. The oncologist prescribed milk thistle but HT was not satisfied and wanted more help. He came to see us.
During his first visit to us, I told HT to go home and think seriously what he wanted to do. Since he has been under the care of an oncologist, there is no reason why he needs our help. Let the doctor repair the so called “damage” because if anything goes wrong later, then someone is going to make us the scapegoat! Remember, this is a Stage 3B cancer. It has spread to the lymph nodes and possible metastasis to the lungs and adrenal gland. The chances of recurrence is very high. And most of the time, if this unfortunate event occurs, people will point their fingers at us — It is because of your herbs! So this is what I told HT. Go home and think about what I have said. I cannot cure your cancer. You can come back again, if you think I can help you.
The next day, HT came back and wanted us to help him — after all, is he not about to fall off the cliff? He has seen his oncologist and was told his liver functions are not good! And he was prescribed milk thistle!
Below is HT’s blood test results over the months.
Table 1: Blood test results up to the 6th chemo.

In January to February, HT had his operation and did not receive any chemo yet. His blood results were good. His blood test results were still okay after 2 shots of chemo. The third shot of chemo lowered his red blood count (RBC) and platelets. This is to be expected — the norm! If the RBC and platelets become too low, the doctor will give you the “red juice” or the “white juice” injection to boost this up again.
Now, let us try to understand what liver function test results tell us.
- Alanine transaminase (ALT). Large amounts of ALT occur in liver cells. When your liver is injured or inflamed (as in hepatitis), the blood level of ALT usually rises.
- Aspartate aminotransferase (AST). When a blood test detects high levels of this enzyme in your blood it usually means your liver is injured in some way. AST can also be released if heart or skeletal muscle is damaged.
- Alkaline phosphatase (ALP). The blood level is raised in some types of liver and bone disease.
- Gamma-glutamyltransferase (GGT). This may be elevated with even minor, subclinical levels of liver dysfunction. It is also raised in chronic alcohol toxicity.
After the third chemo, AST level started to become abnormal and this continued to be elevated throughout and even after the treatment period.
Table 2: Blood test results from the 7th to 12th chemo and 2 months after completion of chemo.
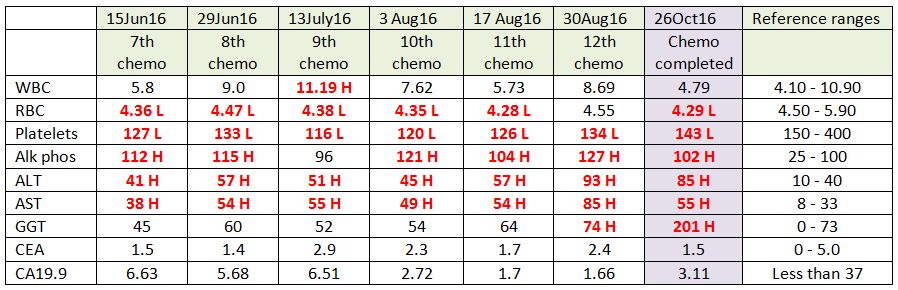
As chemotherapy progressed, HT’s RBC, platelets, alkaline phosphatase, ALT, AST (and later GGT) were adversely affected. We know that the use of chemo-drugs often results in elevated liver function enzymes, which may represent liver toxicity or damage.
In fact, even two months after completion of chemotherapy, HT’s liver function enzymes were elevated. HT started with a good liver, and now has it been damaged by the chemotherapy? Only time can tell what is going to happen next.
Since, HT is worried about this problem, we try to help him by prescribing some liver herbs. Of course, certain people would say, taking herbs would cause more damage to the liver! But, let me tell you, our experience shows otherwise — herbs can repair that damage! Again, only time can tell who is right.
Besides learning the chemo can cause liver toxicity or damage, there are two more lessons we can learn from HT’s experience.
Lesson 1: HT said, initially he was supposed to be operated on by Dr. A but at the last minute he requested to have Dr. B do the operation instead. Why? He did a bit of “homework” and felt that Dr. B is more competent. Bravo! Patients, you must learn to be empowered! Don’t just be led by the nose “to be slaughtered.”
I understand, most cancer patients don’t like to read books or to put it mildly, don’t have time to read books. Let me share with you what I read. Dr. Paul Ruggieri wrote Confessions of a Surgeon, which can give you an insight of what can happen in the operating theatre. He said:
- The “white coat code of silence” is a term I used to describe the dark side of a profession that, despite its noble intentions, enables incompetent surgeons to continue to work.
- The operating rooms are even more insular; there, secrets are often not openly discussed; rarely going beyond the double doors.
- The sad thing was … patients had no idea who they were getting as a surgeon. How does anyone who is about to have surgery truly know how competent the surgeon is? How can the public know?
- Yes, doctors (especially surgeons, because of what they do) are human, and capable of making mistakes. When mistakes are made, people get hurt or die.
- There is no website, no ability to research important, relevant data on your surgeon’s track record before your operation … all we know … he or she has a “good” reputation. Is this enough?
- Hospitals have relevant information … Operating room nurses quickly figure out which surgeons know what they’re doing and which ones should be looking for another profession.
- I believe every person who is about to undergo surgery should have the opportunity to access unbiased performance information about his or her surgeon.
Unfortunately, this ideal is yet to be recongised, let alone practised in hospitals. So, patients, the only way out is for you to use your intuition! If you “feel inside you” that a doctor is not good for you, go find another one!
Lesson 2: I asked HT, How much did he spend for all these treatments — surgery and chemotherapy? He did not know! Because the health insurance paid for everything.
Then HT added, Actually I learned from the Accounts Department that the costs of my treatment were inflated because I have insurance!
Yes, it is common knowledge (not a secret anymore) that if you are insured and landed in the hospital, the treatment charges will automatically sky rocket! While it sounds okay for now, but at the end of it, it is the patients who would suffer from such practice. Your health insurance premium will go up! This unfortunately is one sickness of the health industry which we all know exists but cannot do anything about it!

You must be logged in to post a comment.