AZ is a 45-year-old Indonesian lady. In early 2012, she had a swelling in her left breast. She went to a doctor in Palembang and did a biopsy. The result: not malignant! AZ did nothing after that.
In November 2012, AZ went to a private hospital in Melaka for a second opinion. She was told that she had cancer. A left mastectomy was immediately done on 21 November 2012. It was a Stage 3A cancer. Six out the 16 lymph nodes were found to be infected with cancer. The tumour was positive for estrogen, progesterone receptors and CerbB2 oncoprotein.
AZ underwent follow-up treatments: 6 cycles of chemotherapy, 25 sessions of radiation and was started on Tamoxifen. She had been taking Tamoxifen since 2012 until now.
AZ was well, but was not cured. About four years later, February 2016, AZ felt pain in her left chest. Her surgeon said there was nothing wrong with her! However, AZ consulted another doctor in the same hospital. A lump was found in her chest.
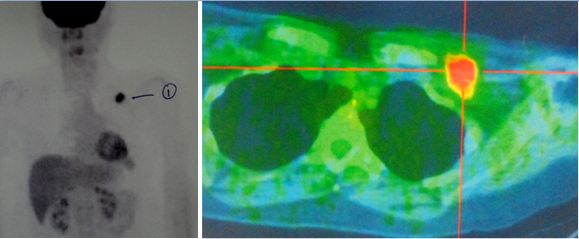
Impression: An active node, probably metastatic, is present in the left supraclavicular region. No other suspicious lesion is detected elsewhere.
AZ underwent another operation to remove the node in her chest. The histopathology report confirmed a recurrent invasive ductal carcinoma. AZ underwent another round of chemotherapy consisting of 6 cycles of oral Xeloda plus 6 cycles of Herceptin. In addition, she received another 25 sessions of radiation.
AZ was told that she had to monitor the progress of her cancer by doing PET scan every 5 months or twice a year!
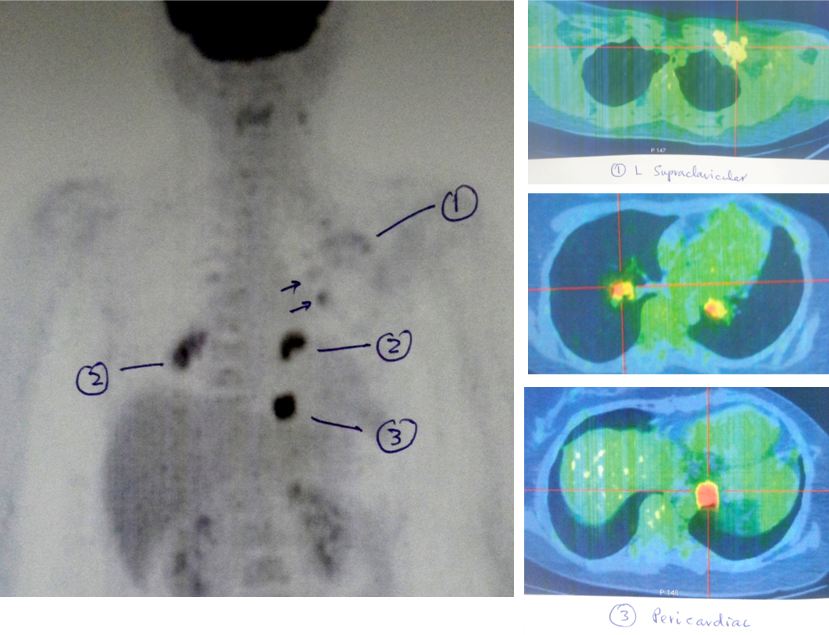
A PET scan done on 24 October 2016, showed more tumours developed. In short, all the previous done failed.
The hypermetabolic node in the left supraclavicular region is much less active.
Two small hypermetabolic lesions have appeared in 2 ribs of the left side.
In the hilar region, there are a few new hypermetabolic nodes of about 1.0 to 2.0 cm.
In the lower mediastinum, there is a hypermetabolic nodules of less than 1.0 cm.
Several small metastases have appeared in the lungs.
AZ was asked to see her oncologist. She refused to return to the hospital again.
Chris: Before the operation, did you ask if surgery was going to cure you?
Patient: The doctor said must operate. Then go for chemo and radiation. Only then can we know if I am going to be cure or not.
C: Did you ask the oncologist, if chemo was going to cure you?
P: The doctor said, “Tak pasti” (not sure!).
PET scan
P: Doctor told me to come back for routine check-up and do a PET scan every 5 months.
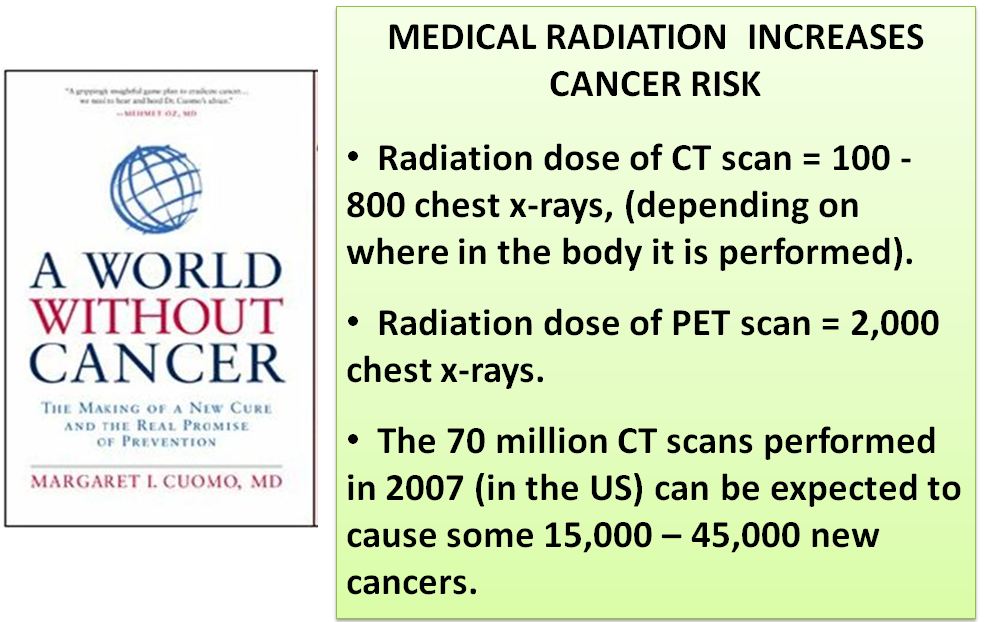
C: What? Every 5 months? Do you know about radiation risks? If I ask you to go for a chest X-ray one time today, is that okay? Yes. But if I ask you to go for an X-ray 800 times a day, you will say I am mad, right? What if I say go 2,000 times of chest X-rays today. I must be real crazy.
Total cost of treatment
C: For all the treatments that you have undergone, how much did you have to spend?
Husband: About RM 200,000.
C: Wah, that is about the cost of a piece of land or a house?
H: Yes, the cost of a house.
Don’t want to see my oncologist anymore
C: What did the doctor want you to do now?
P: I don’t want to do anymore chemo — so far not effective at all. I don’t want to go back and see my doctor anymore. I suffered when I did the previous chemo.
C: I understand. And are you still taking the Tamoxifen?
P: Yes, until yesterday.
CA Care Therapy
C: Who ask you to come here?
H: A friend from Jambi. He had lung cancer and came to see you. Followed your therapy and he is now well — healthy.
C: You need to know that there is NO cure for cancer. I cannot cure your breast cancer. I don’t want to mislead my patients about this. But if I can help you to live a healthy life without problem, then that may be possible. You cannot ask for more. The doctor said you can eat anything you like. No, I am going to tell you that you have to take care of your diet. You cannot eat anything you like. Keep to a healthy diet and lifestyle. What I can do is to try and help you but you must learn how to help yourself. As to how long you live, God decides.
Yoke (not real name, H-469) was a 54-year-old female. Sometime in October 2010, she had on and off pains in her abdomen. Later, the pains extended to her lumbar region. The pains deprived her of sleep. Yoke went to a private hospital for a checkup. Ultrasound, CT scan and blood tests were carried out.
Blood test showed CEA = 38.3 (high); CA 19.9 = 40,003.44 (high); Total bilirubin = 4.6 (low) and GGT = 72 (high).
Ultrasound done on 22 November 2010 showed: “hypoechoic lesion in the pancreatic body … measuring 5.8 x 4.4 x 2.6 cm. There are multiple, well-defined hypoechoic nodules in the liver – the largest seen in the right hepatic lobe, measuring 2.5 cm. Impression: pancreatic body hypoechoic mass is likely a neoplastic lesion with metastases in the liver.”
For confirmation, a CT scan was performed the next day, 23 November 2010. The report indicated: “hypodense mass on the body / tail of the pancreas – measuring approximately 6 x 3 cm. The second hypodense nodule … is also seen more distally in the pancreatic tail. There are a number of hypodense lesions in the liver – the largest lesions are in segment 8, measuring 2.5 cm each. Other lesions are in the caudate lobe, segment 7 and segment 5.
Impression: Carcinoma of the body and tail of pancreas with infiltration of the splenic vein, encasement of the roots of the portal vein and multiple hepatic metastases.
Surgery was not indicated in this case, since the cancer had already spread to her liver. The only option left was to undergo chemotherapy. Yoke was told that she needed to receive seven weekly cycles of chemotherapy. With such treatment, Yoke was told there would be a sixty percent chance of suppressing the cancer (whatever that means?). The oncologist also said that the smaller tumours would not spread after the chemo-treatment.
Yoke refused chemotherapy. She came to seek our help on 20 November 2010. She presented with the following:
Pain in the abdomen and lumbar region. She had to take the painkiller, Tramadol.
Unable to sleep if there were pains.
A bit tired.
She was prescribed Capsule A and B, LL-tea, Liver 1 and Liver 2 teas, Pancreas 1 and Pancreas 2 teas, and Pain Tea.
A week on the herbs: Yoke felt more “cheng sin” (more energetic). Her sleep improved. In the first four days taking the herbs, Yoke suffered the healing crisis. She had intense pains. But the pains gradually subsided and by the fifth day the pains were gone.
Two weeks on the herbs, 10 December 2010: Yoke informed us that she had totally stopped taking the Tramadol prescribed her doctor. She did not have any more pains but she continued taking the Pain Tea. Her sleep was good. Her appetite improved.
Three weeks on the herbs, 17 December 2010: Yoke stopped taking the Pain Tea. And she did not suffer any pain. She said she was always felt hungry after taking the herbs. Our answer to this “problem” – go ahead and eat!
Yoke appeared to be doing well with the herbs. She was then busy making arrangements for her daughter’s wedding. We did not get to see much of Yoke for some months even though we knew that she still continued taking our herbs.
About six months later, May 2011: Yoke came to our centre and she was in severe pains. Why and what had happened?
Yoke said her friend encouraged her to go for a PET scan in order to know what was going on inside her. After all she had been doing well. So Yoke went for a whole body PET/CT scan without seeking our advice. This procedure cost her RM 4,662.
Immediately after the procedure, Yoke suffered severe pains in her abdomen and lumbar region. It was back to the same old problem again.
Let Yoke explain what had gone wrong.
Our conversation
Chris: You went to do a PET scan?
Yoke: Yes and the doctor asked me to eat meat for two days. I was told not to eat rice, fruits, juices and vegetables. I must eat only meat, egg, mushroom and porridge. I was asked to eat these for two days before I went for the scan.
Did he tell you why you need to do that?
So that the pictures would come out clearer.
Did you suffer after taking all these food?
Yes after I took meat, I started to have pains – more pains.
How much did you have to pay?
I put in RM 5,000 and I got back RM 338 (so the cost of her PET scan was RM4,662). If I knew all these, I would not have gone for the scan. They asked me to eat meat for two days – damn it!
But why did you go and do it in the first place>
I have a group of cancer friends. They too went for PET scan. They told me CT scan is not clear and PET scan is clearer – you will know if the cancer is active or not.
So, you follow their advice?
Yes, I was real dumb and went for it.
There is no” meaning” for you to do that!
As you had said. I had pains after that and they could not “repair” me. I had more pains and I was also not able to sleep. More problems for me.
Daughter: They said the cancer had spread to the liver.
Yes, we already knew that anyway. And they asked you to take meat?
That was why the cancer became more active.
They Asked Me to Go for Chemotherapy
They asked me to go for chemo. But the doctor said this was not going to cure me – only maintain. The doctor also said only 25 percent of patients who had chemo lived for two years. So I asked what happened to the remaining 75 percent – “went off”? When the cancer recurs, I would need to do more chemo. No, no – I told the doctor I do not want any chemo. When I told him that, he ignored me – not interested to talk to me anymore.
Let me ask you this – let’s assume that you have two years to live with chemo, and you only have one year if you take herbs. Why one would you choose?
I want to take herbs. May be I might just die sooner with the chemo. I told the doctor, “I might just die while undergoing chemotherapy.” He said, “No, no such thing. I would give you the drug bit by bit.” But I did not want to hear from him anymore.
She Died Soon Afterwards
After the PET scan, Yoke had pains and these got worse by the day. She was unable to sleep or walk by herself, and became weaker. Her stomach was bloated and she was in severe pain. Finally she died not long afterwards.
Information about PET scan from the Internet
X-ray, CT scan and MRI show the anatomy and structure of the organs examined. In contrast, PET scan reveals the metabolic activity and function of the organs. So, X-ray. CT and MRI scans assess the size and shape of different organs in the body. They do not assess function. While a PET scan looks at the body or organ function.
When we go for an X-ray, x-rays are generated from a machine and these rays go through our body and an image is formed on a film. In PET scan a radioactive material, called a radiopharmaceutical or radiotracer, is injected into our bloodstream. The commonly used radiotracer is fluorodexoyglucose (FDG). This is a glucose molecule which has been tagged with a small amount of radioactive element. The radioactive glucose is taken up by cancer cells. Tissues that are active accumulate a large amount of the radiotracer and they show up as “hot spots.” Thus, hot spots indicate high level of chemical or metabolic activity. Less intense areas, or “cold spots,” indicating a smaller concentration of radiotracer and less chemical activity.
PET scan is now considered a new technology. It helps doctors to locate the presence of cancer/infection anywhere in the body. Because cancers are multiplying and require energy for growth, PET scan is designed to detect any mass that is growing fast. The PET scan can also detect the spread of cancer in other parts of the body.
Do you learn any lesson from Yoke’s story?
Yoke learnt her lesson the hard way. Unfortunately it was too late. But can you learn any lesson from Yoke’s experience?
Ask these questions:
The doctor asked Yoke to eat meat, eggs, etc., so that the “picture” will come out clear and nice? Do you know the reason for this after reading the information above? Was he not trying to “wake up the sleeping cancer cells” to make good pictures? It is good for him but this caused more harm to the patient.
What is the “useful” purpose of doing the PET scan anyway – in this case?
To have supportive friends is great but some can lead you to your doom. So before you embark on something, read first. If you cannot read – ask those who really know!
About a year ago, a lady from a neighbouring country urgently flew to see me. She came to discuss the CT scan results of a VIP (very important personality). The CT scan clearly stated that this VIP had tumours in his lungs and liver. His doctor suggested immediate surgery. This lady wanted my advice.
Just to be on the safe side, I suggested that it might be a good idea to know the extent of possible metastases – if at all there is any spread – before undergoing surgery. Towards this end, I suggested that he goes for a PET scan. At that time, my impression was that the PET is the state-of-the-art imaging procedure. It is more accurate and reliable than the CT scan.
After a few days, I was informed by phone that the PET done did not show any malignancy – no cancer! Nevertheless, I hesitated to believe the result. At that time, I “interpreted” the message differently. I had the impression that this VIP wanted to avoid any dealing with me and therefore the only polite “save face” strategy was to tell me that there was no cancer. So he does not need my help anymore!
Some months later, I got to know through another person that this VIP had undergone a liver surgery. This planted the first seed of doubt in my mind about the reliability of PET scan.
Patient from Kelantan
In October 2011, I received a fax from a patient in Kelantan. This 47-year-old male patient did a CT scan on 22 August 2011. The results indicated:
Three well-defined heterogenously hypodense small liver lesions in segments 2, 7 and 8. The largest in segment 2 measuring 0.7 x 1.0 cm. Foci of non-enhancing calcification seen in segment 8 with no mass effect, likely to represent old infection.
Small, well-defined lung nodule seen in the anterior segment of right upper lobe of 0.3 cm in diameter. A small pleural-based nodule is also seen in the posterior segment of left lower lobe measuring 0.3 cm in diameter.
Well-defined small sclerotic bony lesions see in at right acetabulum, left ilium and left neck of femur likely to represent bony island. Multilevel degenerative of the visualized spine.
Impression: Known case of sigmoid colon carcinoma with liver and lung metastases.
This same patient went to do a PET scan in Kuala Lumpur on 5 October 2011. The PET scan result indicated the following:
There is normal uptake in all the organs examined, in particular the colon, liver, lungs, lymph nodes, spleen, pancreas, kidneys, adrenal glands, brain and bones. There is no pleural effusion or ascites.
Impression: No malignant lesion is detected.
This was the second alarm bell. However, I did not take this episode to heart because the patient did not come to see me personally and I did not get to see the images of both the scans. As such I do not have any “solid” evidence to back up what I say – although I did have the faxed reports of both the procedures.
Patient from Penang
The third alarm bell – on 5 February 2012. A man came to our Centre with the medical reports of his wife who has ovarian cancer. She underwent surgery – TAHBSO (Total abdominal hysterectomy with bilateral salpingo-oophorectomy) – on 15 September 2010. This time I had the opportunity to examine the images of both the PET and CT scans.
Six months after the surgery, a PET scan was done at a private hospital in Selangor on 19 April 2011.
Technique: PET scan was performed from the vertex of the skull to the thighs after intravenous administration of 8.5 mCi of F-18 Fluorodeoxyglucise (FDG). Oral gastrograffin, oral bromazepam and intra-venous lasix were given. Fasting blood glucose – 6.9 mmol/l/
Findings:
Head – There is normal physiological localization of the FDG in the cerebrum and the cerebellum. The uptake and the distribution of the radiotracer in the posterior nasopharyngeal tissue, salivary gland and tonsils are within normal physiological limits.
Neck –The thyroid gland displaces normal FDG upake. There is no FDG avid cervical lymphadenopathy.
Thorax – Normal FDG uptake is seen in both breasts. There is no FDG avid axillary lymphadenopathy, bilaterally. There is no FDG avid mediastinal lymphadenopathy. Thre is no pleural effusion seen.
Abdomen – There is no suspicious FDG avid lesion see in the liver. U[take and distribution of the radiotracer in the gallbladder, spleen, adrenals, pancreas, kidneys and bowels are within normal physiological limits. There is no FDG avid abdominal lymphadeopathy. Ascites is not present.
Pelvis – TAHBSO noted. There is no definite abnormal FDG lesion seen in the pelvic floor and vaginal stump. There are some superficial subcentimetre size non-FDG avid inguinal nodes which are likely to be reactive nodes. There is no FGD pelvic lymphadenopathy.
Musculoskeletal – There is symmetrical FDG avid activity seen in the acromioclavicular joints bilaterally, probably due to imflammation. There is no suspicious FDG avid lesion seen in the visualized skeleton.
Conclusion;
There is no evidence of residual hypermetabolic disease in the vaginal stump and pelvic floor.
There is no evidence of hypermetabolic loco-regional or distant metastatic disease at present.
Although there is no evidence of macroscopic disease at present, the presence of microscopic disease cannot be excluded.
The above report was signed by the Consultant Nuclear Medicine Physician.
Three months later, 25 July 2011, this same lady did an ultrasound of her abdomen and pelvis at the same private hospital in Selangor. The results indicated:
Mild ascites is seen.
A thick layer of lobulated parietal pleural masses are seen subdiaphragmatically, around the liver edges superiorly and laterally.
It measures up to 6 x 3.5 cm around segment 8 of the liver and 4.5 x3.7 cm superior to segment 2.
Intrahepatically, a hypoechoic nodule measuring 15 mm is noted in segment 3.
There are also intraperitoneal mesenteric deposit, measuring up to 3.6 x 2.8 cm in the right lumbar territory.
The uterus and ovary absent.
Impression: Extensive intraperitoneal metastases with ascites. Significant progression of the metastasis is seen.
On 16 November 2011, a CT scan of this same lady was done at a private hospital in Penang. The results indicated:
Extensive lobulated hypodense mass noted in the peritoneum and mesentery of upper abdomen.
The mass measured approximately 25 to 65 mm in diameter each.
The mass creep in between the diaphragm and the dome of the liver with marked subcapsular compression of liver.
Masses also noted in the lesser sac and the para-splenic space.
Moderate ascites.
Previous hysterectomy.
Impression: In view of the clinical history, features are consistent with relapsed of carcinoma of ovary with extensive peritoneal and omental metastasis.
Let me end with another story. There was this man who had stomach cancer. After surgery he came to seek our help and was started on the herbs. According to him, he felt good. He liked gardening and used to bring a lot of hot “cabai burung” whenever he came to our centre. He knew that I like hot chilly. One day this patient came and told us that he just had just done a scan and his doctor told him he had no more cancer – everything was clean. So he did not want to take any more herbs – after all the doctor said he was already cured! Although I did warn him that there is no such thing as a cure! No, his doctor’s words were more powerful and after all this was what every cancer patient wants to hear anyway.
A few months later, someone showed me his obituary in the newspaper. Besides learning that he was dead, I also learned that this man was a Datuk – a titled, respected personality in the community.
From the above stories, I learned that we can cause grave danger to patients by telling them things that they only want to hear. Or sending them for test that can give results that they are looking for – of course, the more high-tech the equipment involved, the more convincing it would be. So danger is not only confined to giving them the “wrong kind” of medication – the more toxic the more dangerous.
In this case the lady patient above had a choice – to believe that she had NO cancer after her surgery. What a great relief and welcoming news when the high tech state-of-the art technology similarly confirmed this belief. The lady also had another choice – to believe that surgery did not in any way cure her cancer and actually there were a lot more of the cancer cells left behind after the surgery! High tech gadget was unable to detect that but intuition and plain old-fashion experience is able to decipher that possibility.
Incidentally, while writing this article, I was also reading this humorous, oft-quoted all-time favorite book written by Dr. Oscar London, M.D., the pseudonym of an internist practising in Berkeley, California.













You must be logged in to post a comment.