Doris was a 46-year old lady. Sometime in December 2000 she experienced an excruciating pain in the right shoulder. The pain persisted and a full medical check up indicated serum alpha fetoprotein at 171. A CT scan showed a huge mass in the liver. Doris was asked to go to Singapore for a liver surgery.
On 30 December 2000, 70% of her right liver was excised. Then, she underwent chemotherapy in February 2001. Her surgeon told her that she needed only one cycle of chemotherapy. The surgery cost Doris about S$30,000 and an additional S$10,000 for the chemotherapy.
Doris felt well after all these treatments. She had good appetite but she was bothered by the loss of her hair and distended stomach. She was optimistic having been given such a high hope by her doctors and believing that they had a magic bullet and wonder cure.
29 March 2001 proved to be a very sad day for Doris. An ultrasound showed a moderately enlarged spleen measuring 16 cm. Also there were residual tumours in the remnant of liver parenchyma. A follow up CT scan done on the same day showed at least three, less than 10 mm round hypodense nodules seen in the left lobe of the liver. The spleen is enlarged. In short, the cancer had come back.
Doris came to see us on 29 March 2001. Since she only had 30% of her liver left, we requested that she take only one-third of the normal dose of our herbs. However, Doris did not continue taking the herbs. After about two months on the herbs she switched to Gerson Therapy.
A CT scan done on 28 May 2001 showed presence of three nodules in the remaining liver … the largest nodule was in the upper section and measured 4.5 cm. The other nodules, 2.5 cm and 2 cm were located in the lower sections. The second diagnosis: multicentric hepatoma in previously resected liver.
In the first week of August 2001, barely eight months after everything said and done, Doris died.
Comments
Doris came to see us in Penang. She was indeed a pleasant lady to talk to and help. But we knew there was that much we could do to help. There was already a tumour recurrence in the liver when she started to take the herbs.
Doris underwent an extensive liver surgery in search for a cure but it was sad indeed that she failed to have even a fighting chance, let alone a cure. The surgeon in Malaysia considered her case inoperable because the tumours were more than one. He gave Daisy a year to live. However, the surgeon in Singapore was more heroic. He removed almost 70% of Daisy’s liver, followed by chemoembolization. And the end result, Daisy died 8 months later, instead of 12 months if she was to do nothing.
Perhaps, there is one thing we can learn from this case. No matter how encouraging and heroic your doctor would want to be, resecting 70% of the liver would not make sense. Sometimes it is better to do nothing than to do something.
This is a fax we received from Hong Kong in August 2002.
Dear Dr. Teo,
I am 44 years old. I suffered from cancer of the breast – infiltrating ductal carcinoma in August 1993. Total right mastectomy was performed, secondary to the bones was detected at the same time. Twelve chemo-injections were given over a period of six months. At the same time, radiotherapy was given to the spine and ribs. Two doses of strontium were given after the course of chemotherapy. Tamoxifen and orimetene were taken orally daily all these years.
Everything was in stable condition until August 2001, when secondary to both lobes of liver was discovered. Chemotherapy – FAC, six injections were given followed by eight doses of taxotere.
Now both my lower limbs are swollen. I suffer from pleural effusion at the same time. I started on oral chemotherapy – Xeloda on 10 July 2002. My limbs feel numb. I feel tired easily and my heart sometimes beat irregularly. I feel short of breath at times.
I hope Dr. Teo will help me.
Point to Ponder: All the weapons of war against breast cancer had been used. There are many lessons to learn from her case.
a) Is she winning the war? Is she getting any better or is she getting worse?
b) Can medical treatment cure cancer?
c) Tamoxifen is a proven, liver-cancer-causing drug. She has been taking it for years. What do you think about that? At the end, what did it do? Why the liver cancer?
d) She suffered pleural effusion, i.e, water filling up the lungs. Why is it so?
She was prescribed herbs. And she responded well.
Fax on 22 August 2002: The doctor has stopped giving me Xeloda till my blood test results improve. I have been taking your medicine for 3 weeks. My lower limbs and right upper arm are still swollen. Occasionally I have pain which is similar to electric shock which lasts for a few seconds. This happens only in my swollen limbs. The numbness in my extremities still exists. My heart beats vigorously sometimes but my breathlessness has improved. My general condition is alright and I could go to work as usual. I would like to thank Dr. Teo for taking care of me and hope you could continue helping me.
Fax on 27 September 2002: The doctor gave me Xeloda again for 2 weeks. I dare not refuse because he will close my file and I have no one to turn to when problems arise. Dr. Teo is too far away for me to consult if emergency arise. My lower limbs are back to normal, only swell slightly in the evening but will be alright after a night rest. My right upper limb is still swollen. The axillary lymph nodes were removed in 1993. Is that the cause of the swelling? Physically I am alright.
Fax 2 August 2003: I have stopped taking Xeloda since September. Now I only take your herbal teas and Yunzhi tablets. I am doing alright at the moment, just feeling “pin and needle” in my fingers and feet. I told my doctor here that I am taking your herbs. I would like to thank you again for helping and treating me and keeping me in good general condition. My sincere thanks again.
Fax 3 June 2005: Please advise me as to whether I need to take Bone herbs. This was not prescribed in May 2005. Recently I was suffering from left sciatica and cramps. X-ray of the pelvis showed secondary deposits in the right acetabulum but I didn’t suffer from any pain on my right pelvis at all … I went for a detoxification course in Taiwan during March 2005. I suffered from left sciatica during the course. Physiotherapy didn’t help at all. Dr.Chris, I feel that my heart beats very fast intermittently but ECG was normal. Besides all those mentioned, I am doing fine. Thanks for your kind attention and help.
Fax 30 November 2005: I am physically alright except for my left sciatica. I went to consult a Chinese physician regarding my sciatica. He prescribed Chinese herbs for me to take but I dare not take it … Dr. Chris, what can I do to improve it? …. Other than that I am doing very well. Thank you for helping me all these years. I really appreciate your kindness and helpfulness. I would like to wish you and your family a Merry Christmas and a Happy New Year.
E-mail 26 March 2006: Dear Dr. Chris. I had my blood test done on 15 March 2006. Most of the results turned out within normal range … except CA 15.3 = 5.4. I am quite worried about the rise of CA 15.3. What does the above result indicate?
In mid-2008, after communicating with the patient for 6 years, we flew to Hong Kong and met up with her for the first time. Listen to what she has got to say.
Quotations
In 1993, when I was first diagnosed with cancer, the doctor said: If there is a 1% chance of recovery, I will tell you.
Her doctor was told that she was / and is, taking herbs. It has been 13 years since she was first diagnosed with cancer. During a routine visit to see her oncologist, this was what the doctor said to her:
Oh, I am so surprised that you can walk in after so many years.
Positive words can comfort and heal, but negative words can destroy and kill. Our advice to everyone is, If you have nothing good to say to the sick, you do more good to keep your mouth shut. It helps the sick and at the same time your words may bounce back and make you appear like a fool some day.
Video 1: Nini (M596) is a 38-year-old female from Indonesia. In September 2008, she found a lump in her left breast while bathing. This was diagnosed as adenocarcinoma. In January 2009, she went to Guangzhou, China for treatment. An imaging procedure, done on 14 January 2009, showed a lump about 1.8 x 2.6 cm in size. Pathological study indicated infiltrating lobular carcinoma, Stage 2.
In China, Nini underwent a radical mastectomy. Axillary nodes (0/4) were negative for cancer. Immunohistochemistry indicated ER and P53 negative, PR and HER-2 positive.
After the surgery, Nini received 3 cycles of intra-arterial chemotherapy using Cytoxan or cyclophosphamide, epirubicin and 5-FU. The first two cycles were alright but during the third cycle Nini suffered alarming side effects and she decided to stop the treatment. She was asked to undergo radiotherapy (25 times). She refused. She was asked to take tamoxifen. She refused.
Nini found CA Care and came to see us in Penang on 1 July 2009. She learned about CA Care from a patient in China. When she returned one of her customers brought a book, Kanker Mengapa Mereka Hidup (Cancer Why They Live). She was amazed at this coincidence.
Video 2: While bathingNini heard a voice whispering into her right ear asking her to feel her left breast. She automatically placed her hand on her left breast and felt a lump. She went to seek the advice of the best doctor in town and was told that it was a carcinoma. She decided not to seek treatment at the local hospital.
Video 3: With the help of a friend Nini had an appointment to see a doctor in Singapore. However, another friend told her not to go to Singapore for treatment – nine of ten patients who went there did not make it – they died. She was told to go to China instead. So to China she went.
Video 4: Nini underwent intra-arterial chemotherapy and she described the procedure in detail.
Video 5: Before going to China, Nini read about chemo side effects from books. And when she received chemotherapy in the hospital in China, she felt unhappy with the treatment. After the third chemo, she decided to go home immediately, not wanting to continue with the treatment anymore.
Video 6: The doctor told Nini and her husband that surgery would provide a 100% cure of her breast cancer. But it was not to be. She had to undergo another surgery a month after her mastectomy. Nini refused and felt cheated.
Video 7: Nini suffered some side effects of chemotherapy. Twice her tongue became short or shrunk. This happened after the first and the third chemo. Besides that Nini suffered chemo brain after chemotherapy.
Video 8: When asked how she felt having lost a breast, Nini replied that it was okay after having had an assurance from her husband.
It is unfortunate that the doctor had found it fit to say that surgery could provide a 100% cure for breast cancer. The fact is, surgery does not cure cancer if it has already spread.
A month after the mastectomy, lumps were found in her left armpit and also right neck. The doctor suggested another surgery. Nini refused. This problem became a source of concern for Nini. To find some peace, Nini went to Bali to learn how to meditate. She felt better and more at peace.
When asked if the doctor had ever asked Nini to take care of her diet, the reply was: No, eat anything you like. We cautioned Nini not to believe such an advice. She needs to take care of her diet, which she already did after reading some books.
Our final advice to Nini: Follow what your heart says
Fay discovered a small lump in her breast in April 2000. She did not seek medical help immediately but opted to take herbs instead. A year on herbs and a change of diet did not make the lump go away. Disappointed, she gave up herbal therapy and went on to eat anything she liked. The lump in the breast flared up and became very itchy. Fay decided to undergo a lumpectomy in July 2001. This was followed by fifteen times of radiation. She declined chemotherapy but took tamoxifen for two months and then stopped. She switched to CA Care Therapy in January 2002, i.e., taking herbs and changing her diet and lifestyle. It has been seven years and Fay has led a normal, happy and healthy life.
On 27 August 2007, we requested Fay to share her healing experience with us. The following are excerpts of our conversation.
After removing your lymph nodes, what else did the doctor want to do?
He wanted me to do radiation and chemotherapy. One of my relatives knew this doctor. We also found out that the treatment at the University Hospital (UH) was cheaper. So, I requested him to write me a referral letter to UH. He wrote the letter for me.
What happened at UH?
I saw Dr. N. She was quite a young lady. She said since my cancer was Stage I, I need to do radiation and chemotherapy. But I told her: If it is Stage 1, why must I do chemotherapy? If you want, you can do radiation for me. No need for chemotherapy. Dr. N looked at my file and said:Okay. We’ll do the radiation, fifteen times.
Why did you not want to do chemotherapy?
Because I did not want to lose my hair. I saw my sister-in-law – all her hair dropped. Patients in the oncology ward were all bald. I did not want to go through that.
If chemotherapy did not cause “baldness”, perhaps you would have gone along?
Yes. That was the reason at that time. I did not know then that all these chemo-drugs were so toxic.
How did you get to know us at CA Care?
One day my sister brought a photocopied book, Food & Cancer that you wrote. This was given by her friend, Raja Mariam (you and I do not know her). My sister and I were looking at the book. Then my sister said: We should follow what the book says about cooking oil. Since the CA Care centre is just nearby she asked me to go over and get the original copy. I came and met Khadijah. I cannot remember what she told me, but she also asked me to take the herbs. I explained that I may not be able to afford them. But she asked me not to worry about it. I took the herbs home and consult my sister and brother-in-law. I asked Tok (brother-in-law) whether the herbs were appropriate for me.
You brought back the herbs and asked Tok about them?
I said: I heard that these herbs can cure cancer. He said: Ya. Ini baik. (Yes. This is good. Note: Tok is a Muslim spirit and he talked Malay through Fay’s brother-in-law).
Then I said: I heard that tamoxifen is not good. If I take it, may it cause uterine cancer? He said:Lama-lama boleh jadi. Ini tamoxifen jangan makan. (After some time, this can happen. Do not take tamoxifen.) When I asked what to do with the tamoxifen he had blessed, he replied: Take the tamoxifen that I have blessed for three months. After that, do not take the tamoxifen anymore. Take the herbs instead.
That was what you did. You took tamoxifen for three months?
Yes. He asked me to take the herbs. They would cure my cancer.
After being told all these, how did you feel?
I felt comforted. I did not go back to the oncologist anymore. I believed the herbs would help me.
Siew was 55 years old when she detected a small lump in her right breast. Prior to this event, she was on HRT (hormone replacement therapy) for two years. Siew consulted two doctors about the lump. One doctor brushed her off saying: Since there is no pain, there is nothing to worry. Come and see me only if you have pain. Another doctor, a surgeon did a botch biopsy – taking off only a part of the tumour in her beast. Disappointed, Siew left the matter as it was until the remaining tumour in her breast grew bigger and her breast hardened.
After six months the same surgeon called and warned Siew that the cancer could kill her. This awakened Siew to the seriousness of her problem. She sought the help of another breast surgeon and underwent a mastectomy. After the surgery she was asked to undergo chemotherapy. Siew hesitated and asked if she could seek other options instead. This compassionate doctor did not object to alternative treatment. Siew was subsequently referred to us and was started on herbs inSeptember 2002. She has been on herbs ever since. It has been more than six years and Siew is doing fine.
Medical reports
29 November 2001: Right breast lump biopsy: The tumour cells are seen close to the resected margins. Diagnosis: infiltrating ductal carcinoma, Grade 2.
19 July 2002: Right breast: 2 solid lesions with ill defined borders at 9 o’clock region close to the nipple region. Each measuring 12 x 13 mm and 7 x 6 mm.
7 August 2002: Right breast tumour 2.5 cm, infiltrating ductal carcinoma, grade 2. Surgical margins are clear. Three out of 17 axillary lymph nodes contain metastatic ductal carcinoma.
On 23 December 2007 we interviewed Siew. Below are excerpts of our video-taped conversation:
At this point in time, how do you consider your health? Are you healthy?
Yes. I can do whatever I like. I can clean my whole house by myself. I have no problem with that.
In these five years since your diagnosis, did you ever feel sad thinking of your cancer?
Initially, yes – but now no more.
Did you ever think that you might get a recurrence?
No, never thought of that. Of course I know I have a serious disease, but it did not occur to me that I will die of it. But whenever I hear of people get a relapse, I thought there is also a possibility that it could be me. But, I do not dwell on it. I just think of the possibility of me getting a recurrence.
Looking back at all that you have done … would you go on HRT?
No. I will not take the hormone pills.
If a lady has a lump in her breast like you did, what would you advise her to do?
I would recommend her a certain doctor. But if she is not happy with the doctor, she must seek a second opinion. Do not do what I did – simply follow whatever the doctor said without finding out more.
From the time you found the lump, would you do things differently from what you did?
Yes. I would find a better doctor who could remove the lump completely with a clean margin (lumpectomy). Then I may not have lost my breast at all.
What if after removing the lump, the doctor asked you to go for chemotherapy and radiotherapy? Would you follow his advice?
Unless I know about someone who can take care of me, like you and CA Care and if I have no choice, I would follow what the doctor advised. If I have to choose between herbs and medical treatment, I would definitely choose herbs. I’d always wanted to take herbs. I do not want chemotherapy. If I don’t know about CA Care, then I cannot help it. Even after five years taking the herbs, I still wanted to continue taking it. As for the taste, I still find it very strong despite taking it for so long. I have not grown accustomed to it. (Laughingly)
Besides taking the herbs, you had to change your lifestyle and diet. Were you angry with us about that?
No. I accepted what must be done for my own good. Of course, initially I complained about the difficulty I encountered – having to change the way I used to cook, and what I could eat. But I did not blame you. It is part of the healing path. Also, I did not realize that there was sea-salt which I could use to replace the normal table salt. So, all my food was without salt. It was so difficult to eat as I found the food tasteless. As I visited CA Care centre more often, I learnt about the sea-salt, the liquid amino and the different ways of healthy cooking. Things brightened up and I was happier. Now, I have no more problems preparing my food.
How long did it take for you to get used to the changes?
About half a year.
You were supposed to take herbs, change your diet, exercise and learn to relax. Which is the most difficult thing to do?
The most difficult thing was taking the herb – Breast M Tea. Whenever I took Breast M, my tongue goes le le le le (demonstrating with tongue moving up and down quickly and laughing gleefully).
You have taken the so called “unproven” path for your healing, were you harassed or under pressure by anyone about this?
Yes. My relatives asked: Are you sure the herbs are that good? Can the herbs be trusted? Must you abstain from so many foods? Must you go through so much difficulty? They would urge me to eat whatever they cook even when I told them I have to abstain from those foods. They then told me: No need to abstain from anything. You eat vegetables. Vegetables also have poison(pesticides).
Do you believe them?
They can say what they like, but I do not listen to them. I do not believe what they say. Why must I listen to them and change my ways? I am so well up to this day. Why must I change and take chances. So, I told them that because of the herbs I am taking, I have to abstain from all those forbidden food. This is to cut short the discussion and having to explain so many things to them why a healthy diet is so important in the healing of cancer.
If we were to say: You can now eat whatever you like. Would you?
No. I would not. Not the oily and deep fried food. I can see how bad they are now, such food like satay. Children love it. Now we know how unhealthy it is. As for me, I would not take even a piece of meat.
You win because you are not calculative. You listen to advice. And most of all you are willing to change. Your willingness to change is important.
Speaking of change, my husband’s brother-in-law said: You stupid girl. Cannot eat this, cannot eat that, and cannot eat everything.
Lian was 57 years old when she came and see us. Sometime in 1996, she underwent a hysterectomy. She was put on hormone replacement therapy (HRT). Three years later, she suffered left breast cancer. She underwent a mastectomy in July 1999. It was a medullary carcinoma with no metastasis. She was asked to undergo chemotherapy but declined. She took tamoxifen.
Lian came to see us in November 1999 and was started on the herbs. She then decided to stop taking tamoxifen. It has been 10 years since she was diagnosed with breast cancer. She is doing well and has no problems whatsoever. She is very much alive!
Pathology Report: 27 July 1999: Left breast lump – 3 x 2 cm. Case of medullary carcinoma.
Blood Test Results
——————-Dec. 99 Aug. 03 July 06 Nov. 08
ESR 12 16 19 25 H
Haemoglobin 13.3 14.5 14.0 13.8
Platelet 302 365 330 302
WBC 4.8 5.3 5.5 5.9
CEA 1.0 0.9 1.0 1.5
CA 15.3 n/a 11.1 10.4 14.5
Comments:
Lian is indeed a sweet and pleasant lady. She speaks softly and is totally ignorant of what she is up against, perhaps due to her lack of education. She is a person who follows and fears authority. As such she follows instructions well. She takes her prescribed herbs very religiously and also keeps to her diet.
Lian declined further medication after coming to see us. She did not want any chemotherapy or tamoxifen any more. We could still remember this frail looking lady who came to see us 10 years ago. We could not imagine how she could survive the chemotherapy if she were to undergo the treatment. The side effects of chemotherapy are not like ant bites as some were told. Even without chemotherapy and tamoxifen, Lian does not suffer metastasis. Over the 10 years that she is on herbs, she has not encountered any discomfort or illness at all.
Although Lian is not an educated lady, she has the courage and the commitment to take a different path to healing. She is well rewarded for that adventure. Lian is not alone to try this adventure. There are many others like her. But we do not advise you to embark on a similar journey if you do not believe in what we do or have the commitment to help yourself. Success does not come easy, and there is no magic bullet for cancer.
In Lian’s case we can see the evil in HRT. She ended up with breast cancer. This is not an isolated case linking breast cancer and HRT. We have come across many cases such as this.
Chau (not real name) is a 43-year old female from Johor. She had a lump in her right breast. A biopsy indicated cancer and subsequently she underwent a mastectomy. Chau was indeed in a dilemma when she came to see us. Her 47-year-old sister also had breast cancer. She underwent surgery, chemotherapy and radiotherapy and within a year was dead. Chau was under intense pressure because her oncologist insisted that she undergo chemotherapy and radiotherapy after her mastectomy. She and her brother came to seek our help in May 2004.
I remember saying this to Chau: Don’t worry. I do not think that you are going to die within a year like your sister. Of course, I cannot guarantee that because I am not God. But my experience with breast cancer showed me that even if you do NOTHING, you will not die of breast cancer within a year.
Chau was started on the herbs and was told in no uncertain terms that she must keep to the good diet. I also asked her to go for a blood test, as a baseline for monitoring her progress. Six months on the herbs Chau came back to see us again. I told her: if you live another 6 months, then it means that we are doing the right thing. Remember, your sister died about a year after chemotherapy and radiotherapy.
Chau came to see us again in April 2005. It was almost a year after her initial visit. She was doing well but was very unsettled and concerned as her doctor was still insisting that she go for chemotherapy. I told her: It has to be your choice! Why do you need chemotherapy or radiotherapy? Your sister had chemotherapy and radiotherapy and she died. Remember what Einstein said: Insanity is to do things over and over again and expecting different results. If you do the same things as your sister did, you might end up with the same result – dead.
Pathology Report: 27 April 2004
Infiltrating ductal carcinoma of breast. Size: 1 cm in diameter. Histologically grade 2. Margins of excision are close to tumour. One of 10 axillary lymph node is positive for metastatatic deposits.
Blood Test Results
May 2004 Sept.05 Sept 06
ESR 23 H 4 12
Haemoglobin 11.6 12.1 13.3
Platelet 240 199 228
WBC 3.89 6.9 6.1
CEA 1.0 0.6 0.5
CA15.3 4.4 4.9 5.4
As I am writing this article, Chau’s brother called – what a coincidence! He told me Chau is in perfect health. And this is January 2009, meaning Chau has been well (minus having to endure the agony of the intended toxic treatments) for almost 5 years now. There is every reason to believe and hope that she is going to be able to live for many more years to come.
Comment: We are grateful to God the Almighty that Chau is still alive and well. This is what all patients should feel – be grateful. Chau took a different healing path from her elder sister. However, it is most unfortunate that she had been put under a voodoo curse – without chemotherapy or radiotherapy she would not be cured. There is no truth in such an assumption.
May (not real name) was a 55-year-old lady. Her husband had died of a heart attack three years before, at the age of 62. May was diagnosed with right breast cancer in 2000. She underwent a mastectomy followed by six cycles of chemotherapy. After that she was put on tamoxifen. Three years later, the cancer spread to the right side of her breast in spite of the fact that she was on tamoxifen all these years. May underwent another six cycles of chemotherapy followed by twenty sessions of radiotherapy at the neck and breast areas. Unfortunately, the cancer spread to her neck. She underwent another four cycles of chemotherapy.
From July 2005 to March 2006, she was put on the oral drug, Femara. Then from April 2006 to July 2006, she was on Xeloda.
Her daughter told us that May suffered unbearable pains. When she could not stand the pains she just took off her clothes and ran around the house. At one time May tried to jump out of the window to commit suicide. The arms and areas of her breasts and shoulders were turgid and hard. She felt hot inside. She decided to give up further medical treatment and sought our help at the end of July 2006. The following pictures can tell a better story about her agony.
Comments
Andrew Weil (in Health and healing) wrote: There is never ending struggle … patients are sucked into same way of thinking … finding themselves more and more dependent on the system giving one treatment after another.
Professor Jane Plant (in Life in your hands) wrote: This sounds like a battle between the disease and the treatments – with the patient as the battle ground …Conventional cancer treatment can process patients to the extent that they no longer understand what is really being done to them.
Dr. Lai Gi-ming, Taiwan Cooperative Oncology Group, National Research Institute said: The thing that most frustrates modern doctors is that, after surgery, chemotherapy and radiotherapy, all they can do is keep chasing and chasing the cancer!
(Life on earth is a living experience. Let the death of Fransiska be a lesson for many of those who come after her).
Fransiska, from Jakarta, was thirty-two years old when she found a 1.6 cm lump in her left breast which was diagnosed as cancer. At about the same time, her father had died of cancer. In November 2004, she underwent a lumpectomy in a Singapore hospital. Unfortunately some lymph nodes in her arm pit were also infected. After surgery, Fransiska received thirty-five radiation treatments. She was well after the treatment.
In January 2007, i.e., two years after the radiation treatment, Fransiska was told that her cancer had spread to her lungs. She underwent chemotherapy and received six cycles of Taxol and injections of Herceptin. Each Herceptin injection cost S$2,500 and Fransiska had eight injections. Her oncologist thought she should continue with Herceptin but she decided to stop after eight injections because she could not afford to pay for the treatment anymore.
In July 2007, Fransiska was put on tamoxifen. A month later, a bone scan showed the cancer had spread to her spine, T 12.
In January 2008, a brain scan showed a 8 x 7 mm mass in her brain. There was also a 1.4 x 9.0 cm mass in her liver. Fransiska was asked by her doctor to stop taking tamoxifen. She was prescribed oral chemo-drugs – Xeloda and Tykerb (lapatinib). A three-week treatment of Tykerb cost S$2,500.
Fransiska told us that she was aware of the “bad effects” of medical treatment but she had no choice. She did not know what else to do except to seek doctors’ advice.
In November 2004, Fransiska started on a juicing program with apple, beet root and carrot (ABC). She also took apricot seeds (source of Vitamin B17), cloves, black walnut tincture and wormwood. In addition she took IP6, spirulina, Perfect Food and high dose Vitamin C. She stopped all these intake in 2007 when the cancer had metastatised to the lungs.
In February 2005, she underwent a detoxification and rejuvenation program with ABC juicing and coffee enema. She continued to do this until she found traces of blood in her urine. She stopped this program.
Fransiska also took pineapple and papaya.
Fransiska was aware of the need to eat healthy food. She was on fruit and vegetable juices, and she avoided white sugar, oil, egg, all meat and processed food. She took shark cartilage but later stopped it because it was not effective.
She suffered headaches, nausea and had very low blood pressure. Fransiska went back to her oncologist in August 2008. A scan showed the cancer had spread to her brain. A CT scan of the abdomen showed:
metastasis in both hepatic lobes. The largest lesion in the left lobe measures 2.0 x 1.8 cm and the largest in the right lobe measures 1.5 x 1.4 cm.
Sclerotic focus in the T12 vertebral body is stable.
The oncologist concluded that the disease had progressed and suggested two options:
Fransiska undergoes more chemotherapy in addition to taking Lapatinib, or
She continues taking Lapatinib; receives regular injection to strengthen her bone and take medication to relieve her menopausal symptoms. Earlier, Fransiska was treated with Zoladex to stop her menses.
Fransiska wrote me often to ask for help. The last email I received from her was on 30 October 2008 when she complained of gastric problem. It is with sadness that Fransiska slipped into coma and she died 2 days later, mid-December 2008. Her death came four years after being diagnosed with breast cancer. Even the most expensive and up to date drugs for cancer could not save her.
Comments:
This is a tragic story indeed but which has been played over and over again – breast cancer turned Stage 4 and incurable. What has gone wrong? In fact, nothing had gone wrong! Fransiska followed what her doctor wanted her to do. She received the state-of-the-art medical treatment inSingapore. Yee, a 40-year-old lady from Penang also died in similar way. She had an early stage breast cancer. Underwent surgery, chemotherapy, radiotherapy, took tamoxifen and Tykerb besides receiving Herceptin. She ended up with mestatsis to the lungs, bone, live and eventually brain. She died after spending more than RM 100,000 for the treatment.
At CA Care, over our thirteen years of experience, we observed three phenomena that tend to occur among breast cancer patients.
1. One, our data show that breast cancer patients (in Malaysia) who underwent surgery, chemotherapy, radiotherapy and took tamoxifen suffer metastasis to the bone, lung, etc. after a few years. Those patients (in Indonesia) who turned to traditional medicine or who did not receive the standard medical treatment did not suffer much metastasis or suffered metastasis much later.
2. Young patients who underwent a full package of medical treatment for breast cancer tend to suffer severe metastasis.
3. Now with the availability of Herceptin, we begin to see patients suffering from brain metastasis. Is there any correction between this treatment and brain metastasis?
We recognise that our observations are anecdotal and therefore can be disputed. A search in the net yielded some results which are indeed worthy to take note of.
The Boston Globe (A new peril for breast cancer survivors by Liz Kowalczk, 7 February 2006) carried a story of Amy Socia who was diagnosed with breast cancer when she was 43 years old. She underwent a mastectomy, breast reconstruction surgery, radiotherapy and chemotherapy. In spite of the medical treatments the cancer spread to her liver and spine. Amy was prescribed the so-called promising drug – Herceptin – and “miraculously” her cancer began to shrink! But it was not to be. Not long afterwards (five years after her initial diagnosis) two tumours appeared in her brain. This led Amy to conclude: “There is no cure for metastatic breast cancer. It never goes away. You just move from treatment to treatment.”
Amy’s story is not much different from Fransiska’s.
Fransiska was treated with lapatinib (Tykerb) and capecitabine (Xeloda).This modern treatment have been shown in one study “to shrink brain metastasis significantly in six percent of 241 patients.” In the official lapatinib website: www.tykerb.com, we can read the following information:
There is no cure for metatastatic breast cancer, but it can be treated.
Some women may develop liver damage while taking Tykerb. In some cases, liver damage may be severe and may cause death.
The side effects of Tykerb include: nausea, vomiting, heartburn, loss of appetite, red, painful hands and feet, rash, dry skin, sores on the lips, mouth, or throat, pain in the arms, legs, or back, difficulty falling asleep or staying asleep, shortness of breath, cough, coughing up pink or bloody mucus, fast, irregular, or pounding heartbeat, tiredness or weakness and swelling of the hands, feet, ankles, or lower legs.
Patients need to remember that to be able to treat cancer does not mean cancer can be cured! To cure is to spend a lot of money but the treatment does not cure. Shrinkage of tumour is also not a cure! Lapatinib causes liver damage. Is this not what happened in Fransiska’s case?
The side effects of Herceptin include: Fever and chills (commonly occur during the first treatment), breathing and heart failure, diarrhoea, headache, nause and vomiting, pain, skin rash and weakness. However, what are most disturbing are reports about Herceptin and brain metastasis.
A report dated 13 December 2001 by Robert Carlson stated:
It is known that patients with metastatic breast cancer are more likely to develop bone metastasis but patients who recive Herceptin appear to be at increased risk of subsequent development of brain metastasis compared to bone metastasis.
The journal, Cancer (15 June 2003, Vol: 97:2972-2977), stated:
Metastatic breast carcinoma to the CNS (brain) is common among patients receiving Herceptin.
Approximately 6 to 16% of women with metastatic breast carcinoma develop brain metastasis but patients who received Herceptin as a first-line therapy had a high risk of developing CNS (brain) disease (42%).
The question we may wish to ask: how relevant is the above observation to Fransiska’s brain metastases? What could have happened with Fransiska did nothing – would she die of breast cancer within four years?
Tin (M597) was 38 years old in 2007 when she found lumps in her breasts during a regular medical check up. A CT scan done on 21 May 2007 indicated: no lung nodules or abnormal masses or enlarged lymph nodes.In the left axilla are slightly prominent lymph nodes – these are under 1 cm in size. There are no liver lesions seen.
Tin underwent a left mastectomy on 1 June 2007. The histology report indicated:
Right breast biopsy – fibroadenoma in background of fibrocystic disease.
Left breast (biopsy and mastectomy specimen): multifocal ductal carcinoma in-situ with invasive ductal carcinoma; invasive carcinoma measures 4.3 cm in maximum diameter; DCIS and invasive carcinoma extend close to the deep resection margin; skin and nipple are not involved by tumour.
Left axillary lymph nodes: 4 out of 6 lymph nodes contain metastatic carcinoma, with extracapsular spread.
TNM classification: pT2N2aMx, Stage 3A.
The tumour is negative for oestrogen and progesterone receptors, weakly reactive to C-erb-B2 and strongly reactive to P53. These results suggest that the breast cancer is unlikely to respond to tamoxifen / endocrine therapy.
As with most cancer patients, Tin underwent chemotherapy and radiotherapy after the surgery. Her husband was not sure how many courses of chemotherapy Tin had received. But one thing was sure – she was not getting any better. The oncologist behaved gently and encouraged Tin to continue taking the chemotherapy in spite of her deteriorating condition. She had full faith in her oncologist. According to her husband, Tin received Avastin towards the end of her chemo-treatment. Tin also underwent radiotherapy but her husband could not remember how many times she received the radiation treatment.
A follow up CT scan on 14 May 2008 indicated: no lung nodules or masses seen. Mediastinum remains clear of mediastinal lymphadenopathy. Liver also remains clear of metastatic deposits.
CT scan on 17 February 2009 indicated:
Multiple pulmonary metastases are noted. This shows interval increase in size and number when compared with previous CT dated 22 December 2008.
There is also interval development of bilateral pleural effusions, left larger than the right.
Mediastinal and bilateral hilar lymphadenopathy are seen. This is unchanged when compared with previous CT. There is however interval development of left axillary nodes.
There are now several small subcentimeter hypodense lesions seen in the liver compatible with hepatic metastases. These are not present in the previous CT.
CT scan on 8 June 2009 indicated:
There is extensive pleural shadowing seen in the lung fields on both sides with evidence of associated effusions noted.
This is associated with lung nodules in both lungs the largest of which measures approximately 1 cm in the mid zone of the left side.
A small associated pericardial effusion is seen.
In the lower cuts, the liver outline shows no abnormalities.
Tin’s husband and mother-in-law came to seek our help on 2 July 2009. This is the gist of what we were told.
Tin’s husband and mother-in-law did not seem to agree that Tin undergo such extensive medical treatment but Tin insisted in carrying out what the oncologist wanted her to do. She questioned:Herbs are not proven, what if I took herbs and these do not work. As a result, her mother-in-law was afraid to give further comment. Even when Tin’s condition had turned worse and she became breathless due to fluid in her lungs and pericardium, the oncologist was saying there was nothing to worry. Every three weeks she had to have a blood transfusion. After Tin gets out of the hospital, the oncologist said she should come back to him for more chemotherapy.
Realizing that she was not going anywhere with medical treatment, Tin as last agreed to try our herbs. This resulted in Tin’s husband and mother-in-law flying to Penang to see us. We prescribed some herbs but expressed our skeptism.
On 19 July 2009, Tin’s husband came to Penang again. He informed us that Tin had been hospitalized and was only able to take the herbs for three days so far. Her condition was deteriorating. The doctor had requested the family to take Tin home. At most she would survive for another 2 months. Tin needed oxygen to help her breathe.
All in all, the family had spent approximately S$200,000 for the treatment. Tin’s husband told us: Please try to save my wife.
Barely 3 days after her husband’s second visit, we received this e-mail:
Wed, Jul 22, 2009 at 5:42 PM
Dear Mrs Teo,
Thank you so far for your help rendered by you and Dr. Teo. This morning at 9:21 am, my wife finally passed away after her struggle against the cancer for this past 2 years. She lost her battle ….
Comments: Is losing a battle against cancer such as this something unusual? Definitely not. At CA Care we witness see such disasters all too often. Tin had undergone all the medical treatments necessary for cancer and she died within two years. Where is the proven science in this case?
Granted, Tin’s cancer was serious – Stage 3A, but her CT scan of 14 May 2008 indicated no problem with her lungs or liver. There were also no serious problems with her lymph nodes. But one a half years later, trouble started brewing. CT scan in December 2008 indicated recurrence and it became even more serious in February 2009 in spite of more treatments (more of different poisons?).
By June 2009 Tin’s condition became more critical and she had fluid in her lungs and also her pericardium (heart lining). What had happened? Was this due to her cancer or the results of her treatment?
Often treatments of breast cancer are referred to as Slash, burn and poison.It is also said that these treatments are worse than the disease. What could have happened if Tin were to do nothing invasive and go for alternative treatment? Having to suffer and to spend S$200,000 but ending up dead within 2 years is no bargain at all.
Dr. Frank Daudert of Pro Leben Klinik in Igls /Innsbruck, Austria said: Doctors give chemo, chemo, chemo. And patients die, die, die. He went on to say: Doctors are blindly giving chemotherapy to some patients while the cancer cells smile and the patients die.
Tin was totally committed to curing her cancer by the medical way. To her, herbalists are quacks and the herbs are not proven. She had resisted seeking alternative therapy or help. According to her family she only agreed to take the herbs in July 2009, and a few days later she died. That was a bit too late! There are many patients who are like her. Let this be a lesson to numerous others who come after her.
Life on earth is a living experience. Let the death of Yee be a valuable lesson for many others who come after her.
Yee was 40 years old when she was diagnosed with breast cancer in October 2005. She underwent a mastectomy. It was a Stage 2 disease with no lymph node involvement. The tumour was 3 x 2 x 2 cm in size.
After surgery, Yee received 6 cycles of FAC chemotherapy (5-FU, Andiamycin and Cyclophosphamide). No radiotherapy was indicated. Chemotherapy was completed in March 2006 after that she was started on tamoxifen.
Yee was well for about 9 months. Sometime in January 2007, she noted a swelling in the right side of her neck. A CT scan of the thorax on 19 January 2007 indicated: multiple nodules scattered in both lung fields ranging from 2 to 10 mm. This means the cancer had spread to her lungs.
Yee was given 8 cycle of taxane-based chemotherapy. This treatment was not effective. CT scan on 4 July 2007 showed the nodules in the lungs were progressing.
Yee received more chemotherapy – 6 cycles of Navelbine + Herceptin. This treatment cost about RM 50,000. CT scan in November 2007 showed stable disease. From November 2007 till December 2008 Yee was on the oral drug, Tykerb (lapatinib) 4 to 5 tablets per day. Each tablet cost RM 65.00. At RM 260.00 per day this medication cost RM 7,800 per month. It seemed that the total cost for about 14 months on Tykerb came to about RM 93,000.00.
By February 2008, failures started to show up again. A CT scan on 13 February 2008 indicated:enlarging pulmonary nodules ranging from 0.5 to 2.2 cm.
Six months later, 19 August 2008, CT scan indicated pulmonary nodules are increasing in number and measure from 0.5 to 5.0 cm. Subcentimeter mediastinal nodes are also seen.
In October 2008, Yee suffered right arm pain and there was palpable swelling in the right collarbone. CT scan on 13 October 2008 showed more serious disease progression:
fibrosis in the right axilla.
an irregular ill-defined node in the right infraclavicular region, approximately 2.0 cm.
another small right supraclavicular node, 0.7 cm is also present.
medistinal nodes,size slightly increased from the last CT examination.
pulmonary masses and nodules are enlarging. The largest mass, in the left lung is currently 5.6 cm. Other lesions measure from 1.0 to 4.8 cm.
A new hypodense lesion, approximately 1.0 cm is now seen in Segment 7. This is suspicious of liver metastasis.
In view of the progressive disease, Yee underwent 28 times of radiation treatment starting 13 October 2008 until 1 December 2008, while at the same time continuing with her oral-drug, Tykerb.
On 17 December 2008, York suffered headaches and was unable to sleep. A CT scan done on 19 December 2008, indicated multiple brain metastases.
Yee and her husband came to seek our help on 5 December 2008. Yee’s condition was serious. Her right arm was numb. She had no appetite. She was severely breathless. Even the supply of oxygen to her nostrils did not help at all. She told her husband she would rather die. In early February 2009, Yee was admitted to the hospital where the doctor suggested that she receive radiation to her brain. It was not to be – she died even before the treatment.
This is a tragic case. Yee’s story is similar to that of Fransiska of Indonesia. Fransiska underwent surgery and received chemotherapy, radiotherapy, Herceptin and Tykerb + Xeloda. Fransiska died. She was diagnosed in November 2004 and died in December 2008. Yee was diagnosed with a Stage 2 breast cancer in October 2005, underwent similar treatments and she died in February 2009.
Doctors, the media and patients always look to newer drugs and newer technologies as a new hopefor treating illnesses. We have been hooked and made addicted to the idea that somethingnew is always better. Herceptin and Tykerb are new bullets for cancer which are now beginning to appear in our local landscape. Are they better or dangerous?
There is no cure for metastatic breast cancer. But it can be treated. What do you by such a vague treatment? Surely we can treat anything if there is money!
Some women may develop liver damage while taking Tykerb. The cause of this damage is not known. Liver damage may be severe and may cause death.
The most common side effects of Tykerb are diarrhea; vomiting; feeling sick to your stomach; feeling tired; red, painful hands and feet; and rash.
Dry cough or have shortness of breath may be signs of inflammation in the lungs.
1. Herceptin can cause heart muscle damage that can lead to heart failure.
2. Herceptin can also affect the lungs, causing severe or life-threatening breathing problems.
3. Herceptin can cause allergic reactions that can be severe or life-threatening. Symptoms of a reaction include a drop in blood pressure, shortness of breath, rashes and wheezing.
4. Because of these potentially life-threatening side effects, doctors are WARNED to evaluate patients carefully for any heart or lung problems before starting treatment. Do you think they ever do this? In this case, Yee had metastasis (that is not severe problem enough?) to her lungs. As such would Herceptin not make things worse for her? When she came to us she was severely breathless. What could have been the cause?
And one most important question which patients (and doctors?) do not even care to ask: Does Herceptin cure breast cancer? The answer is absolutely NO. Addition of Herceptin to the normal chemotherapy regime prolonged survival by 4.6 months. Nowhere in the website ever says that Herceptin cures breast cancer. Read the section: Possible Benefits of Herceptin (take note, even the title itself does not seem to inspire much confidence and hope) in its official website: http://www.herceptin.com/adjuvant/what-is/benefits.jsp
Dr. Ralph Moss wrote a report entitled: Herceptin or Deception. Michael Janson, M.D., past president of the American College of Advancement of Medicine gave this comment about the report: Dr. Mossreveals the hollow core of the recent medical reports on Herceptin, showing that it is not what has been claimed, and that the statistics were manipulated to make it seem far better that it is, while underplaying the potential risks.
In Yee’s case, like in many other cases before her, perhaps there is no point asking the same question: What has gone wrong? Things seem to go wrong most of the time. Allow me to think aloud:How could a Stage 2 breast cancer kill a patient within four years? Would she have died if she was to do nothing?
Breast cancer is less common among those in their thirties, but if breast cancer occurs in younger women, it tends to be more aggressive than in older women. While this may be true, some people want to make us believe that it is because Yee was young and had an aggressive type of cancer that make her treatment ineffective. Let me invite you read the case of three ladies who were before forty when they had cancer yet they survive. The only thing they did differently was that they did not blindly their doctors – they declined chemotherapy, radiotherapy or hormonal treatments.
Tee, a 38-year-old lady who was diagnosed with breast cancer in October 2005 (note: at about the same time as Yee) and she refused chemotherapy. Tee is still alive as of this writing (March 2009) while Yee died in February 2009. You can read Tee’s story in our Case Report series.
Sue was 39 years old when she discovered 2 lumps in her right breast in 2003. She underwent a mastectomy. Her oncologist told her that with chemotherapy she would have 5% chance more of survival. She but declined further medical treatment, including tamoxifen as suggested by her surgeon. Sue change her diet and lifestyle and took herbs. It has been 6 years now and Sue has been leading a trouble-free life.
Julia discovered a 4 cm lump in her breast in 1995. She was then 36 years old. She was asked to undergo a mastectomy. She declined and never went to see her doctor again. She declined chemotherapy, radiotherapy or hormonal therapy and decided to seek alternative healing. She father is an herbalist and naturally she turned to him for help. Julia’s healing journey along the uncharted path is interesting and sometime dangerous. But to fact remains she is still very much alive and well as of this writing (2009). It was 14 years that she was first diagnosed with cancer. The detail story of Julia is found in our book: The herbal option, Chapter 3.
Cindy was 34-years old when she was diagnosed with breast cancer in August 1994. She underwent a lumpectomy. Since the margin was not clear she was asked to undergo a mastectomy to be followed by chemotherapy and radiotherapy. She declined further medical treatment. She changed her lifestyle and diet, did qi gong and meditation and sought homeopathic therapy. It has been 15 years and Cindy has been leading a healthy without any problem (Chapter 2: The herbal option).
Dr. Frank Daudert, Pro Leben Klinik in Austria said: Doctors are blindly giving chemotherapy … while the cancer cells smile. Doctors give chemo, chemo, chemo. And patients die, die, die.
In their book: More harm than good, Alan Zelicoff, M.D., and Michael Bellomo, J.D./MBA, wrote: (Physicians are) taught that doing nothing almost guarantees that the patient will suffer and that doing something outweighs doing nothing. The truth is that the vast majority of cancer – once spread – remain incurable despite the availability of many dozens of new chemotherapeutic drugs and even the use of antibodies directed against cancer cells.
Richard Deyo and Donald Patrick, professors, University of Washington, Seattle, USA, wrote in their book: Hope or hype – the obsession with medical advances and the high cost of false promises: We are born with our own blind trust in a medical establishment that preys on our deepest fears, all the while purporting to ride to our rescue with “miracles cures.” Indeed many medical advances do offer real advantages but there are as many others that offer little, if any, advantage and many have alarming side effects … marginally effective at best – and sometimes downright dangerous …. They often lead to useless, harmful and unnecessarily expensive care … When doctors introduce new products good money often trumps good science.
Fay (not real name) is a 45-year-old Malaysian. She was diagnosed with breast cancer in September 2006.
She underwent a mastectomy with axillary clearance (removal of lymph nodes).
After the surgery she received 25 radiation treatments and six cycles of chemotherapy. The drugs used were 5-FU, epirubin and cyclophosphamide (FEC). All treatments were completed in April 2007.
Every 4 months Fay went back to her oncologist for routine surveillance check up. Everything was alright.
In August 2008, cancer was found in her bones – L2, L5, sacrum and pelvis.
She had been on tamoxifen for almost 2 years (November 2006 to August 2008). Tamoxifen had failed and the doctor suggested that she take another drugs, Arimidex.
She received to receive more chemotherapy and suffered badly from the side effects.
Case 2
Rin (not real name) and is a 40-year-old Indonesian lady living in the United States. She wrote:
First I was diagnosed with breast cancer in December 2004.
I did the lumpectomy on the left breast in February 2005.
After the surgery, I received 8 cycles of chemotherapy. After the chemotherapy I had menopause.
I then had radiotherapy for 35 times and I finished it in October 2005.
I took tamoxifen, 20 mg once a day.
I did regular check up with my oncologist every 6 month and I did yearly mammogram and the past 2 years I also did the bone density test.
In August 2008, I started feeling pain in my left leg and sometimes in my left arm. The pain did not go away and it hurt more and more. Then I was not able to and walk straight and could not bend. It was very hard for me to go up and down the stairs.
In November 2008, I had a whole body scan and also CT scan. The cancer had spread to the bones – left humeral head, left femur and L5.
I again did radiotherapy for the effected area for 10 times.
In Dec 2008, I developed blood clots in my left leg.
My doctor changed my medication from tamoxifen to Arimidex.
Case 3
Gay (not real name) is a 43-year-old Australian. She was diagnosed with breast cancer in 1999. She wrote:
I received 6 months of chemothrapy and 3 months radiation therapy.
Then I was started on tamoxifen for 5 years followed by Arimidex.
I have had no problems until the past 6 months. I had a slight pain in my right upper abdominal. My tumor markers were elevated.
After a number of scans, it turned out to be bone metastases.
Case 4
Sri (not real name), 57-year-old Indonesian, was diagnosed with left breast cancer in 2003. She underwent a mastectomy followed by chemotherapy and radiotherapy. At the time we talked to her, Sri appeared to have chemo brain and was unable to recollect the details of her treatment. Her response to our questions was also very slow. Sri received all these treatments in New Zealand.
Sri went back to her doctor for routine check up and was told everything was fine. However, in 2007, she did not feel well. Further examination indicated bone metastases. She again received six cycles of chemotherapy and 10 radiation treatments. All treatments were completed in November 2008. Sri came to Penang in February 2009 and did a CT scan. The results indicated the following:
Lesion in T1 and T5 vertebrae.
Nodule in C5 and lesion in L4 vertebral bodies.
Several lytic lesions in the left iliac bones.
Suggestive of liver cirrhosis.
What can we learn from these four cases?
1. These patients had undergone all the required medical treatments – surgery, chemotherapy, radiotherapy, and oral drugs – tamoxifen and Arimidex. They had received the best that medical science has to offer but cancer still recurs.
2. Oncologists say all these are treatments are scientifically proven, FDA-approved backed by data reported in peer-reviewed medical journals. The questions are: What is so great about all these? Why do these patients still suffer metastasis? What is the “real and honest” truth about all these treatments?
3. Does it ever cross somebody’s mind that theinability to cure or the ability of the cancer to spread could also be due to the treatments themselves?
4. Look at these cases again. Fay in Malaysia suffered metastasis 1 year and 4 months after completion of her medical treatment. Rin from USA and Sri in New Zealand suffered metastasis barely three years after her treatment while Gay from Australia had metastasis about eight years after her treatment. These cases reflect similar problems faced by most patients everywhere in the world. It does not matter where you live and who or what you are, doing the same thing produces the same results.
Einstein said: Insanity is to the do the same thing over and over again and expecting different results.Can you learn anything from the wisdom of this great Man of Science? Patients in the USA,Australia, New Zealand and Malaysia received the same kind of treatments and all of them ended up with the same results. Over the years, I have observed similar stories being repeated over and over again so much so that bony metastasis can or is expected after such treatments. To expect otherwise is what Einstein said is insanity.
The questions that boggle the mind are: Why are those in the know NOT doing anything about it?Why are patients kept in the dark and not warned about this possibility? Perhaps we can do MORE than just prescribing drugs? Tamoxifen is supposed to prevent recurrence but in all the cases above, it has failed miserably. Why don’t we look beyond what are being done today?
Surgeon told him three years too late that nine out of ten patients whom he operated on died anyway
KB (H467) is a 57-year-old male. In 2006, he suffered back pains. CT scan of the abdomen on 23 June 2006 indicated: “a hypervascular lesion in the right lobe of liver in Segment 6/7 measuring 3.5 x 5.2 x 4.5 cm. This has ill-defined margins. Features suggestive of an underlying hepatoma.” In short, KB had liver cancer and without hesitation and in haste due to fear, he underwent liver surgery in a private hospital in Penang. This cost him RM35,000.
As a follow-up treatment, KB underwent seven times of chemoembolisation. Each treatment cost RM5,000. The first five treatments were well tolerated but the last two caused severe side effects. It was a difficult experience and KB said he was “half dead”.
About three years later, KB felt a lump in his abdomen. CT scan on 23 June 2009 report is a follows:
“There is a previous segment 6/7 and 7/8 wedge liver resections. There are multiple foci of lipiodol uptake in the liver post chemoembolisation in keeping with multicentric hepatomas. These range from 2 – 20 mm in size. There are several recurrent hypervascular foci noted scattered in the subdiaphragmatic region of the right lobe of liver ranging from 5-15 mm. Absent gallbladder (previous cholecystectomy). No evidence of abdominal lymphadenopathy.”
Another CT scan was done on 4 September 2009. The imaging report appeared exactly the same as the one written on 23 June 2009 with the following exception:
“There are several hypodense foci in the right subdiaphragmatic region ranging from 2-15 mm. Impression: several hypodense lesions scattered in the subduaphragmatic region of the right lobe of liver, ? generating nodules, ? early hepatomas.
MRI was also done on 3 October 2009. The report appeared exactly the same as the CT scan reports of 23 June and 4 September 2010, with the following exception:
“There are multiple irregularly enhancing nodules scattered in both lobes of the liver with clustering in the right subdiaphragmatic regions ranging from 3- 20 mm. These are suspicious of multicentric hepatomas.”
It was a real disappointing result for KB and his family. At that time he was still undergoing chemoembolisation. KB complained to the surgeon that the treatment was making him sick. The surgeon said this: “Out of ten patients I operated on, nine died.” KB and his family were also told that KB was already lucky that he is still alive. “Most of others patients have all died. If you do not wish to continue with the chemo, you would be waiting to die.”
Listen to our video conversation below.
The son told us: But he only told us this fact three years after the operation. The surgeon should have told us before he did the operation. Disappointed KB decided to see another doctor in Ipoh. A total body CT scan was done on 10 August 2010. The report is a follows:
“There are multiple hypodense lesions seen within the liver affecting nearly the entire parenchyma, with clustering seen in the subdiaphagramatic region. This is suggestive of multicentric hepatoma. The area of involvement is worse than that seen in previous scans.
In the private hospital in Ipoh, KB received three i/v chemo treatments. Unfortunately the treatment was not effective. The family was told about CA Care and KB and his family came to see us on 26 November 2010. Take a look as his blood test results.
4 Oct 10
15 Oct 10
4 Nov 10
19 Nov 10
Direct bilirubin
7.3
6.7
5.9
7.4
SGOT/AST
116
103
112
132
SGPT/ALT
66
49
55
74
GGT
882
723
649
790
Alkaline phosphatase
179
157
138
179
Alpha-fetoprotein
2480
2419
3185
3208
Comments:
This is indeed a sad story. Talking to KB and members of his family that night, made me realized how vulnerable we all are. KB trusted the expert to cure him. He was willing to spend so much money to find the cure for his liver cancer. He did not doubt about what he was doing – for that matter he probably took it for granted that he would get his cure. Like most people believe, after the operation the cancer is gone.
Then came the bombshell three years too late. He was told that nine out of ten patients who underwent liver surgery died anyway! I asked him: “Before you had the surgery, did you ever ask the doctor if surgery would cure you?” The answer was NO. Well, most patients never ask such a question. They took for granted that surgery would be the “magic tool”. His wife said: “We were ignorant”. KB said: “I was in fear.”
Dr. Hamilton, a neurosurgeon, in his book: The scalpel and the soul, wrote: “As doctors, we generally don’t tell outright lies. We just don’t speak the truth fully.”
So, here it is. If you don’t ask you get no answer. There is a Malay saying: Segan bertanya, sesat jalan (Shy to ask, you lose your way).
This is what I always tell patients. Before you do anything – be it surgery, chemotherapy, radiotherapy or even taking drugs – ask the doctor first of the possible and expected outcome. Why the rush to get things done? Ask if what he is going to do or giving you is going to cure you or not. Then evaluate his answer or response. What he says, how he says it and how he addresses your concern (including his body language) will tell you where you are heading for.
I was a bit baffled that night. I asked KB and his family – what made the surgeon say that damaging “confession” – nine out of ten patients whom he operated on died. In what context or under what circumstance did he say such a thing? I got this answer. KB was unhappy because the chemo was “killing” him and he complained to the surgeon about it. He was reluctant to go on further with the chemo – in spite of having received seven “shots” already. In an effort to make KB comply with his instruction, perhaps “threatening” KB with a possible death would do the trick?
But then why come out with such damaging statement? One is tempted to speculate that this “truth” has been lying buried in his heart all these days of his professional life but he could not share this truth with his patients. But once a while, things have to “explode” and be let out. Unfortunately for KB, this truth is revealed three years too late. What if KB was told that he had only a 10 percent chance of survival before he underwent the surgery? Would he go ahead with the surgery?
Why must doctors adopt the attitude that “we just don’t speak the truth fully”?
At CA Care we lay out our cards on the table – clearly and fully. When KB came to see us, I have made it clear that I would not be able to cure him at all. But I promise to do my best to help him – the way that I know how. I told him to keep to the good diet. Cancer patients cannot eat anything they like. I am aware that most patients are disappointed and they never come back again after hearing my “lecture.” That is okay – it is better to be honest and become unpopular with patients than misleading them. The wise words of Rabbi Harold Kushner came to mind. In this world we have a choice on how we conduct our affairs: “There is the morality of cleverness and wit, in which success means getting the better of the other person by means of a slick business deal or a clever answer. Then there is the morality of righteousness, in which the highest good is thoughtfulness toward others. The worst sin is hurting another person.”
In his book, Never to be lied to again, Dr. David Lieberman wrote:
In an ideal society there would be no need for lies. But we live in a world of deception. And whether you want to play or not, you’re in the game.
And there’s one undeniable truth about lying – everybody does it.
Some of these lies can be “subtle that they can be easily missed unless you pay close attention”. Others may be glaringly obvious. In some instances, you’ll be looking for lies of omission – what’s missing that should be there.
Dr. Lieberman offered numerous tips in his book on how to detect lies and deception. Here are some examples:
Body language – the truth can be always silently observed. No or little direct eye contact is a classic sign of deception. Feeling guilty a lier does not want to look you in the eyes. Liers tend to be less expressive with his hands or arms. Arm movements and gestures seem stiff and almost mechanical – not natural.
Someone who is lying rarely points a finger, either at others or straight up in the air. Finger pointing indicates conviction and authority.
Watch out for the good old Freudian slip or slip of the tongue. This is a subconscious leak when a person’s misspoken words reflect and reveal his true feelings, thought or intentions.
He doesn’t want to respond to a question. He may imply an answer but never answers it directly.
When asked a question, he depersonalizes his answer by offering his belief on the subject instead of answering directly.
Here are something we can do and need to be aware of:
When you’re desperate, you’ll be apt to do what you never should do – make a decision out of fear.
Just because you’re told that something is the latest, best, hottest or biggest seller does not make it right for you.
A white lab coat does not make anyone an expert.
Evaluate a person’s integrity based upon what is being presented not what is promised.
Often we don’t stop and ask ourselves, “Does this make sense?” A dash of common sense can go a long, long way.
We certainly can’t stop people from trying to lie to us, but we can keep them from being successful.
Hass (not real name, M847) is a 44-year-old male from Indonesia. In early 2010, he had jaundice. The doctor suspected this was due to Hepatitis. Hass was prescribed medication. After a month, the treatment was not effective. Hass went to a private hospital in Kuching.
A CT scan on 28 January 2010 indicated a 6 mm stone in the gallbladder. There was a 1 cm hypodense lesion in segment 8 of his liver. This could be just a cyst. The common bile duct was dilated. The maximum diameter was 16 mm. There was a 18 mm mass at the distal common duct. Conclusion: Mass in the lower common duct with biliary obstruction.
Immediately Hass underwent an operation to remove his gallbladder and the bile duct tumour. The histopathology report dated 3 February 2010 indicated: infiltrating moderately differentiated exophytic adenocarcinoma of bile duct, invading through entire thickness of the wall and metastatic to periductal lymph nodes. Margins of excision free of tumour.
An ultrasound of the abdomen on 8 June 2010 showed no evidence of tumour recurrence although his CA19.9 increased from 52.4 (in March 2010) to 1420.0. A CT scan on 9 June 2010 indicated a 15 x 10mm lesion in segment 7 of his liver. The 10 mm cyst in segment 8 of his liver remained the same. In addition there were a few paraaortic lymph nodes noted from the celiac axis down to the liver of the renal hilum. The largest node measured 20.0 mm – the others were subcentimeter.
The doctor told Hass that the cancer had recurred and he was unable to help him anymore. Hass was asked to undergo chemotherapy. But he refused.
Below is a table showing the rise of CA 19.9 markers from March to October 2010.
Date
CA 19.9
Before operation
2,000 plus
18 March 2010 – after operation
52.5
8 June 2010
1,420.0
3 August 2010 – last visit to surgeon
5,645.0
1 October 2010
18,746.18
Hass came to see us in Penang on 8 October 2010. Listen to our conversation.
Review of Medical Literature
Understanding the Liver-Gallbladder-Pancreas-Bile Duct Complex
Attached to the liver, is a pear-shaped structure called the gallbladder.
The liver makes bile and this is transported to the intestine by a long tube-like structure called the bile duct.
The gallbladder is attached to the bile duct by a small tube called the cystic duct.
The top half of the bile duct is associated with the liver while the bottom half of the bile duct is associated the pancreas through which it passes on its way to the intestine.
Blockage of the bile duct by a cancer prevents the bile from being transported to the intestine. When this happens the bile accumulates in the blood giving rise to jaundice. The skin and eyes becomes yellow. This condition may also cause severe itchiness.
(Diagrams are obtained from the internet)
The clinical presentation, prognosis and natural history of bile duct cancer (or cholangiocarcinoma) depend on where the cancer originates. The cancer may occur:
In the part of the bile ducts contained within the liver. This is known as intra-hepatic.
In the part of the bile ducts outside the liver. This is known as extra-hepatic.
In the duct between the left and right portal veins. This is known as hilar bifurcation.
60%-70% of cholangiocarcinomas occurat the hilar bifurcation.
20%-30% inthe distal common bile duct.
5%-15% within the liver (intra-hepatic).
Patients with extrahepatic tumors usually present withpainless jaundice due to biliary obstruction, while patients withintrahepatic tumors usually present with pains, pruritus (66%), abdominal pain (30%-50%), weight loss(30%-50%), and fever (up to 20%).
In their review, Anderson et al also noted that:
The majority of patients with cholangiocarcinoma presents with unresectable,advancedstagedisease and have a survival of less than 12 months. Cure rates are low, even with aggressive therapy. The average 5-year survival rate is 5%-10%.
Surgery remainsthe only intervention offering the possibility of a cure. But the treatment goal should be complete excision with negativemargins.
All patients should be fully evaluated for resectabilitybefore any type of intervention is performed.
Neoadjuvant and adjuvant therapieshave not improved survival in patients withthis tumor.
Since the prognosis for unresectable patients is poor, palliative measures should be aimed at increasing qualityof life first and increasing survival second.
Results of Surgery
Among selected patients who undergo potentially curative resections,5-year survival rates are generally from 8%-44%.
The importance ofachieving a margin-negative resection cannot be overemphasized.The 5-year survivalrates were greater when a negative margin was obtained, 19%-47% versus 0%-12%.
Distal lesions represent approximately 20%-30% of all cholangiocarcinomasand are usually treated with pancreaticoduodenectomy (Whippleprocedure). Achieving a margin-negativeresection is also important with these tumors. The 5-year survival rates in selected patients who underwentcurative resections is21%-54%.
Intrahepatic cholangiocarcinoma is usually treated by hepaticresection. Three-year survival rate of 60% was reported in patients who underwent a margin-negative partial hepatectomy.
Chemotherapy
Chemotherapy has not been shown to markedly improve survivalin patients with either resected or unresected cholangiocarcinoma.The majority of reports use 5-FU alone or in combination withmethotrexate, leucovorin, cisplatin, mitomycin C, or interferonalpha.
The 5-year survival rates were not significantlydifferent between patients who received chemotherapy and surgeryand those who received surgery alone.
Surgery may be used to remove the cancer if it has not spread beyond the bile duct. It is not always possible to carry out surgery, as the bile duct is in a difficult position and it may be impossible to remove the cancer completely.
There are different surgical procedures depending upon how big the cancer is and whether it has begun to spread into nearby tissues.
These surgical procedures are:
Removal of the bile ducts. If the cancer is small and contained within the ducts, then just the bile ducts containing the cancer are removed.
Partial liver resection. If the cancer has begun to spread into the liver, the affected part of the liver is removed, along with the bile ducts.
Whipple’s. If the cancer is larger and has spread into nearby structures, then the bile ducts, part of the stomach, part of the duodenum, the pancreas, gall bladder and the surrounding lymph nodes are all removed.
Bypass surgery. Sometimes it is not possible to remove the tumour. Other procedures may be performed to relieve the blockage and allow the bile to go into the intestine. The jaundice will then clear up.
Stent insertion. One way to relieve jaundice without a surgical operation is to perform ERCP (Endoscopic Retrograde Cholangiopancreatography). This procedure involves insertion of a tube, called a stent into the blocked bile duct. The stent clears a passage through the bile duct to allow the bile to drain away. The tube usually needs to be replaced every three to four months to prevent it becoming blocked. If the tube does block, recurrent high temperatures and/or return of the jaundice will occur.
Non-surgical stenting is regarded as the first choice of palliation for patients with short life expectancy.
For patients with longer projected survival, surgical bypass should be considered.
Palliative resections may be beneficial to patients with distal and hilar bifurcation.
Questions to Ponder
The fact is very clear. Surgery for bile duct cancer in this case is an absolute failure. Is this failure a rare event? Probably NOT! A surgeon told his liver patient: “For ten liver operations that I performed, nine patients died”. Good information indeed but the problem is that he made this comment some three years too late. This patient had already undergone the operation and had suffered a severe recurrence.
A few more questions come to mind:
According to the literature, not all patients with bile duct cancer are suitable condidates for surgery. “All patients should be fully evaluated for resectabilitybefore any type of intervention is performed”. To what extent is this evaluation done?
The surgeon recommended chemotherapy after the recurrence. What benefit can the patient expect from this? Medical literature clearly indicates that “Chemotherapy has not been proven to be of definite benefit.”
Is the suggestion of chemotherapy after the failure of surgery, a way of “passing the buck” to someone else? “I have done my job to cut it out. My responsibility is over. Now you go to the oncologist and see what he can do for you.”
Goh (not real name, H438) was a 36-year-old male. In June 2010 he had diarrhea and his blood pressure was low. He was admitted into a private hospital in his home town. An USG was done and he was told that his liver was not good. After three days he was discharged from the hospital. Health returned to normal. Two weeks later his abdomen became hard. He went back to the hospital again and a CT scan done indicated hepatoma – or liver cancer.
Goh came to a private hospital in Penang. He was asked to undergo surgery, to remove half of his liver. An operation was done but was later aborted. This open-close surgery cost him RM 10,000.
Not knowing what else to do, Goh and his family came to seek our advice on 24 October 2010. His CT scan report dated 15 October 2010 stated: “Both lobes of liver are enlarged and studded with multiple ill-defined heterogeneously enhancing lesions. The largest lesion located in segment 4b measures 15 x 20 x 15.6 cm. Impression: Multicentric hepatoma with minimal ascites and dilated left intrahepatic duct.”
Blood test results elevated liver enzymes. SGOT = 203, SGPT = 56, Alkaline phosphatase = 736 and Alpha-fetoprotein = 213.73.
Goh presented with pains in the shoulder area. These pains only appeared after the surgery. Before that there was no pain. He was not able to sleep. His eyes were blood shot. His abdomen was extended with both legs swollen. His breathing was difficult.
Unfortunately, Goh died not long after seeing us.
Comments: I don’t think it is necessary for me to give any comment on this case. The fact speaks for itself. Goh died barely two months after this aborted surgery. What do you think – would he have died earlier or later if he did not undergo that surgery?
This is one book which I believe everyone should read – Confession of a Medical Heretic by Robert Mendelsohn. The author is not an ordinary man. In the US, he wrote a syndicated column called “The People’s Doctor”. He was an associate professor at the University of Illinois Medical School and a director of Chicago’s Michael Reese Hospital. He was also chairman of the Medical Licensure Committee for the state of Illinois. In Chapter 3 of his book, Dr. Medelsohn wrote:
I believe that my generation of doctors will be remembered for … the millions of mutilations which are ceremoniously carried out every year in operating rooms.
Conservative estimates … say that about 2.4 million operations performed every year are unnecessary.
My feeling is that somewhere around ninety percent of surgery is a waste of time, energy, money and life.
Modern cancer surgery someday will be regarded with the same kind of horror that we now regard the use of leeches in George Washington’s time.
Greed plays a role in causing unnecessary surgery … there’s no doubt that if you eliminated all unnecessary surgery, most surgeons would go out of business.
Ignorance plays a part in a lot of unnecessary surgery.
Greed and ignorance aren’t the most important reasons why there is so much unnecessary surgery. It’s basically a problem of belief: doctors believe in surgery. There is a certain fascination in “going under the knife” … that (surgeon) can overcome anything because he can operate you … “You don’t have to take care of yourself, we can fix you if you go wrong.”
To protect yourself … your first step is to educate yourself. Get a second opinion. If you decide that surgery isn’t the answer, do whatever you have to do to detach yourself from the situation. In any situation short of an emergency, you’ve got plenty of time not only to decide whether or not you need the surgery but also who should perform the operation.

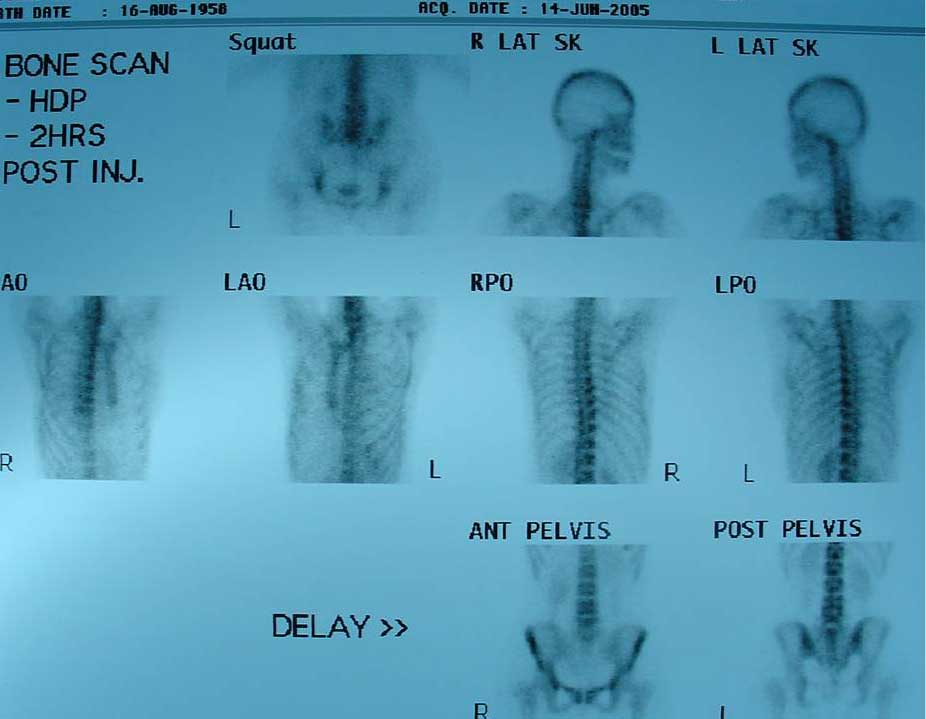






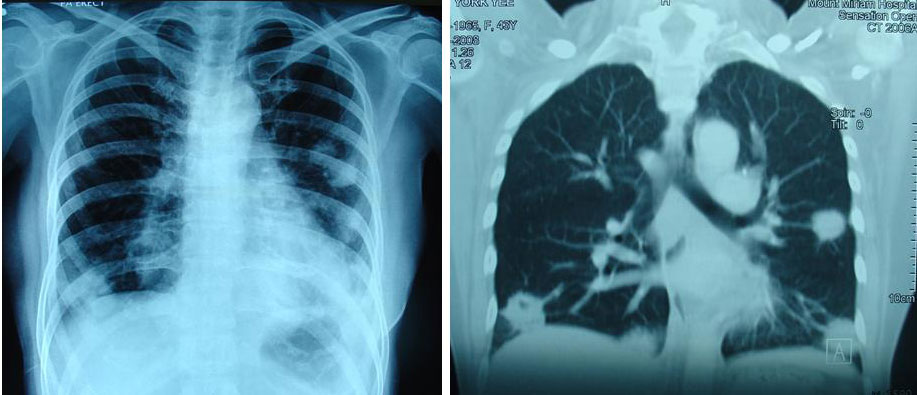
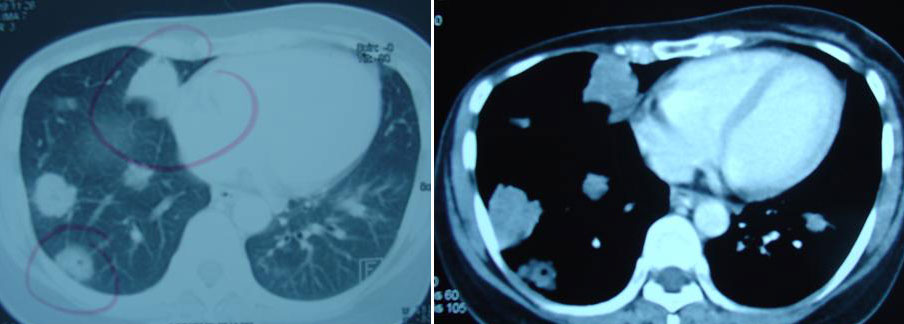

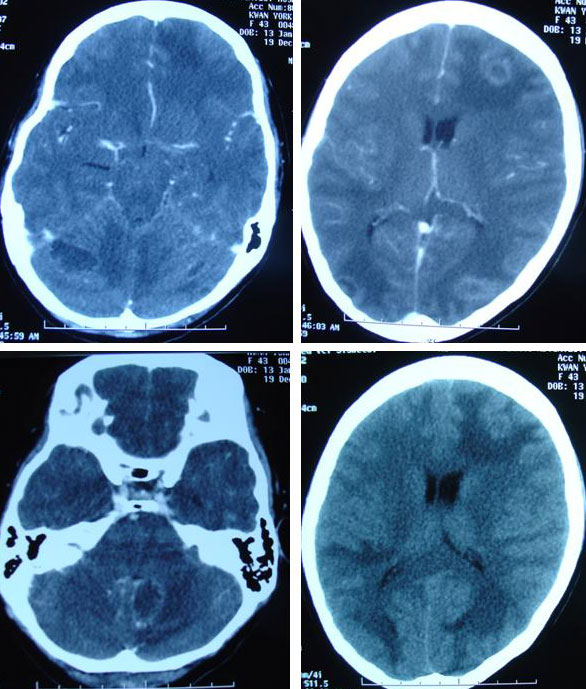
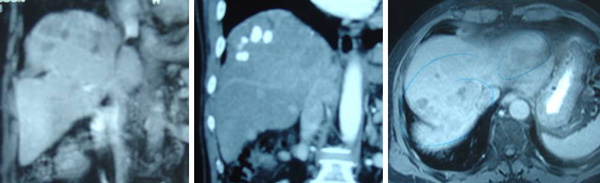




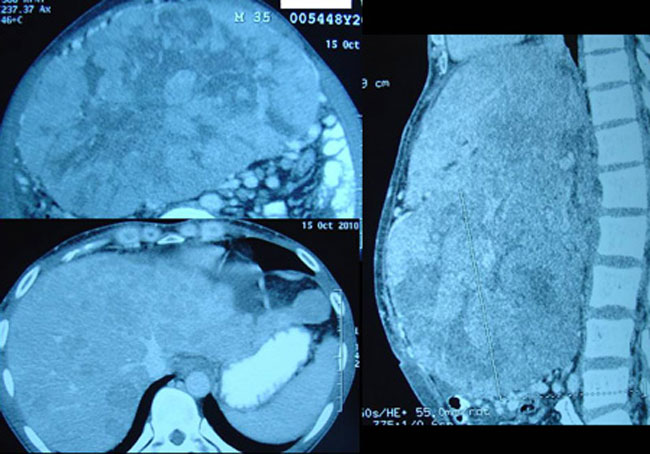


You must be logged in to post a comment.