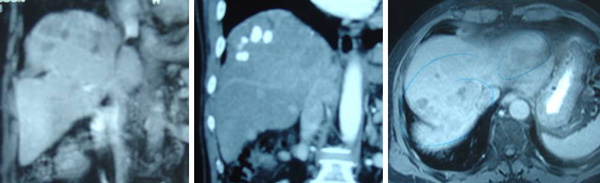
Doris was a 46-year old lady. Sometime in December 2000 she experienced an excruciating pain in the right shoulder. The pain persisted and a full medical check up indicated serum alpha fetoprotein at 171. A CT scan showed a huge mass in the liver. Doris was asked to go to Singapore for a liver surgery.
On 30 December 2000, 70% of her right liver was excised. Then, she underwent chemotherapy in February 2001. Her surgeon told her that she needed only one cycle of chemotherapy. The surgery cost Doris about S$30,000 and an additional S$10,000 for the chemotherapy.
Doris felt well after all these treatments. She had good appetite but she was bothered by the loss of her hair and distended stomach. She was optimistic having been given such a high hope by her doctors and believing that they had a magic bullet and wonder cure.
29 March 2001 proved to be a very sad day for Doris. An ultrasound showed a moderately enlarged spleen measuring 16 cm. Also there were residual tumours in the remnant of liver parenchyma. A follow up CT scan done on the same day showed at least three, less than 10 mm round hypodense nodules seen in the left lobe of the liver. The spleen is enlarged. In short, the cancer had come back.
Doris came to see us on 29 March 2001. Since she only had 30% of her liver left, we requested that she take only one-third of the normal dose of our herbs. However, Doris did not continue taking the herbs. After about two months on the herbs she switched to Gerson Therapy.
A CT scan done on 28 May 2001 showed presence of three nodules in the remaining liver … the largest nodule was in the upper section and measured 4.5 cm. The other nodules, 2.5 cm and 2 cm were located in the lower sections. The second diagnosis: multicentric hepatoma in previously resected liver.
In the first week of August 2001, barely eight months after everything said and done, Doris died.
Comments
Doris came to see us in Penang. She was indeed a pleasant lady to talk to and help. But we knew there was that much we could do to help. There was already a tumour recurrence in the liver when she started to take the herbs.
Doris underwent an extensive liver surgery in search for a cure but it was sad indeed that she failed to have even a fighting chance, let alone a cure. The surgeon in Malaysia considered her case inoperable because the tumours were more than one. He gave Daisy a year to live. However, the surgeon in Singapore was more heroic. He removed almost 70% of Daisy’s liver, followed by chemoembolization. And the end result, Daisy died 8 months later, instead of 12 months if she was to do nothing.
Perhaps, there is one thing we can learn from this case. No matter how encouraging and heroic your doctor would want to be, resecting 70% of the liver would not make sense. Sometimes it is better to do nothing than to do something.
Surgeon told him three years too late that nine out of ten patients whom he operated on died anyway
KB (H467) is a 57-year-old male. In 2006, he suffered back pains. CT scan of the abdomen on 23 June 2006 indicated: “a hypervascular lesion in the right lobe of liver in Segment 6/7 measuring 3.5 x 5.2 x 4.5 cm. This has ill-defined margins. Features suggestive of an underlying hepatoma.” In short, KB had liver cancer and without hesitation and in haste due to fear, he underwent liver surgery in a private hospital in Penang. This cost him RM35,000.
As a follow-up treatment, KB underwent seven times of chemoembolisation. Each treatment cost RM5,000. The first five treatments were well tolerated but the last two caused severe side effects. It was a difficult experience and KB said he was “half dead”.
About three years later, KB felt a lump in his abdomen. CT scan on 23 June 2009 report is a follows:
“There is a previous segment 6/7 and 7/8 wedge liver resections. There are multiple foci of lipiodol uptake in the liver post chemoembolisation in keeping with multicentric hepatomas. These range from 2 – 20 mm in size. There are several recurrent hypervascular foci noted scattered in the subdiaphragmatic region of the right lobe of liver ranging from 5-15 mm. Absent gallbladder (previous cholecystectomy). No evidence of abdominal lymphadenopathy.”
Another CT scan was done on 4 September 2009. The imaging report appeared exactly the same as the one written on 23 June 2009 with the following exception:
“There are several hypodense foci in the right subdiaphragmatic region ranging from 2-15 mm. Impression: several hypodense lesions scattered in the subduaphragmatic region of the right lobe of liver, ? generating nodules, ? early hepatomas.
MRI was also done on 3 October 2009. The report appeared exactly the same as the CT scan reports of 23 June and 4 September 2010, with the following exception:
“There are multiple irregularly enhancing nodules scattered in both lobes of the liver with clustering in the right subdiaphragmatic regions ranging from 3- 20 mm. These are suspicious of multicentric hepatomas.”
It was a real disappointing result for KB and his family. At that time he was still undergoing chemoembolisation. KB complained to the surgeon that the treatment was making him sick. The surgeon said this: “Out of ten patients I operated on, nine died.” KB and his family were also told that KB was already lucky that he is still alive. “Most of others patients have all died. If you do not wish to continue with the chemo, you would be waiting to die.”
Listen to our video conversation below.
The son told us: But he only told us this fact three years after the operation. The surgeon should have told us before he did the operation. Disappointed KB decided to see another doctor in Ipoh. A total body CT scan was done on 10 August 2010. The report is a follows:
“There are multiple hypodense lesions seen within the liver affecting nearly the entire parenchyma, with clustering seen in the subdiaphagramatic region. This is suggestive of multicentric hepatoma. The area of involvement is worse than that seen in previous scans.
In the private hospital in Ipoh, KB received three i/v chemo treatments. Unfortunately the treatment was not effective. The family was told about CA Care and KB and his family came to see us on 26 November 2010. Take a look as his blood test results.
4 Oct 10
15 Oct 10
4 Nov 10
19 Nov 10
Direct bilirubin
7.3
6.7
5.9
7.4
SGOT/AST
116
103
112
132
SGPT/ALT
66
49
55
74
GGT
882
723
649
790
Alkaline phosphatase
179
157
138
179
Alpha-fetoprotein
2480
2419
3185
3208
Comments:
This is indeed a sad story. Talking to KB and members of his family that night, made me realized how vulnerable we all are. KB trusted the expert to cure him. He was willing to spend so much money to find the cure for his liver cancer. He did not doubt about what he was doing – for that matter he probably took it for granted that he would get his cure. Like most people believe, after the operation the cancer is gone.
Then came the bombshell three years too late. He was told that nine out of ten patients who underwent liver surgery died anyway! I asked him: “Before you had the surgery, did you ever ask the doctor if surgery would cure you?” The answer was NO. Well, most patients never ask such a question. They took for granted that surgery would be the “magic tool”. His wife said: “We were ignorant”. KB said: “I was in fear.”
Dr. Hamilton, a neurosurgeon, in his book: The scalpel and the soul, wrote: “As doctors, we generally don’t tell outright lies. We just don’t speak the truth fully.”
So, here it is. If you don’t ask you get no answer. There is a Malay saying: Segan bertanya, sesat jalan (Shy to ask, you lose your way).
This is what I always tell patients. Before you do anything – be it surgery, chemotherapy, radiotherapy or even taking drugs – ask the doctor first of the possible and expected outcome. Why the rush to get things done? Ask if what he is going to do or giving you is going to cure you or not. Then evaluate his answer or response. What he says, how he says it and how he addresses your concern (including his body language) will tell you where you are heading for.
I was a bit baffled that night. I asked KB and his family – what made the surgeon say that damaging “confession” – nine out of ten patients whom he operated on died. In what context or under what circumstance did he say such a thing? I got this answer. KB was unhappy because the chemo was “killing” him and he complained to the surgeon about it. He was reluctant to go on further with the chemo – in spite of having received seven “shots” already. In an effort to make KB comply with his instruction, perhaps “threatening” KB with a possible death would do the trick?
But then why come out with such damaging statement? One is tempted to speculate that this “truth” has been lying buried in his heart all these days of his professional life but he could not share this truth with his patients. But once a while, things have to “explode” and be let out. Unfortunately for KB, this truth is revealed three years too late. What if KB was told that he had only a 10 percent chance of survival before he underwent the surgery? Would he go ahead with the surgery?
Why must doctors adopt the attitude that “we just don’t speak the truth fully”?
At CA Care we lay out our cards on the table – clearly and fully. When KB came to see us, I have made it clear that I would not be able to cure him at all. But I promise to do my best to help him – the way that I know how. I told him to keep to the good diet. Cancer patients cannot eat anything they like. I am aware that most patients are disappointed and they never come back again after hearing my “lecture.” That is okay – it is better to be honest and become unpopular with patients than misleading them. The wise words of Rabbi Harold Kushner came to mind. In this world we have a choice on how we conduct our affairs: “There is the morality of cleverness and wit, in which success means getting the better of the other person by means of a slick business deal or a clever answer. Then there is the morality of righteousness, in which the highest good is thoughtfulness toward others. The worst sin is hurting another person.”
In his book, Never to be lied to again, Dr. David Lieberman wrote:
In an ideal society there would be no need for lies. But we live in a world of deception. And whether you want to play or not, you’re in the game.
And there’s one undeniable truth about lying – everybody does it.
Some of these lies can be “subtle that they can be easily missed unless you pay close attention”. Others may be glaringly obvious. In some instances, you’ll be looking for lies of omission – what’s missing that should be there.
Dr. Lieberman offered numerous tips in his book on how to detect lies and deception. Here are some examples:
Body language – the truth can be always silently observed. No or little direct eye contact is a classic sign of deception. Feeling guilty a lier does not want to look you in the eyes. Liers tend to be less expressive with his hands or arms. Arm movements and gestures seem stiff and almost mechanical – not natural.
Someone who is lying rarely points a finger, either at others or straight up in the air. Finger pointing indicates conviction and authority.
Watch out for the good old Freudian slip or slip of the tongue. This is a subconscious leak when a person’s misspoken words reflect and reveal his true feelings, thought or intentions.
He doesn’t want to respond to a question. He may imply an answer but never answers it directly.
When asked a question, he depersonalizes his answer by offering his belief on the subject instead of answering directly.
Here are something we can do and need to be aware of:
When you’re desperate, you’ll be apt to do what you never should do – make a decision out of fear.
Just because you’re told that something is the latest, best, hottest or biggest seller does not make it right for you.
A white lab coat does not make anyone an expert.
Evaluate a person’s integrity based upon what is being presented not what is promised.
Often we don’t stop and ask ourselves, “Does this make sense?” A dash of common sense can go a long, long way.
We certainly can’t stop people from trying to lie to us, but we can keep them from being successful.
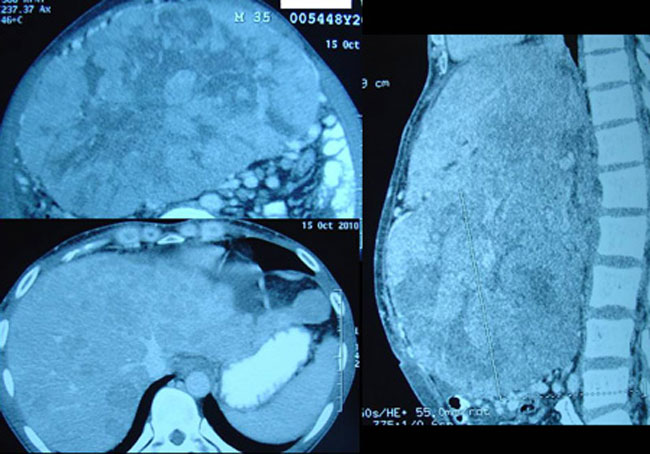
Goh (not real name, H438) was a 36-year-old male. In June 2010 he had diarrhea and his blood pressure was low. He was admitted into a private hospital in his home town. An USG was done and he was told that his liver was not good. After three days he was discharged from the hospital. Health returned to normal. Two weeks later his abdomen became hard. He went back to the hospital again and a CT scan done indicated hepatoma – or liver cancer.
Goh came to a private hospital in Penang. He was asked to undergo surgery, to remove half of his liver. An operation was done but was later aborted. This open-close surgery cost him RM 10,000.
Not knowing what else to do, Goh and his family came to seek our advice on 24 October 2010. His CT scan report dated 15 October 2010 stated: “Both lobes of liver are enlarged and studded with multiple ill-defined heterogeneously enhancing lesions. The largest lesion located in segment 4b measures 15 x 20 x 15.6 cm. Impression: Multicentric hepatoma with minimal ascites and dilated left intrahepatic duct.”
Blood test results elevated liver enzymes. SGOT = 203, SGPT = 56, Alkaline phosphatase = 736 and Alpha-fetoprotein = 213.73.
Goh presented with pains in the shoulder area. These pains only appeared after the surgery. Before that there was no pain. He was not able to sleep. His eyes were blood shot. His abdomen was extended with both legs swollen. His breathing was difficult.
Unfortunately, Goh died not long after seeing us.
Comments: I don’t think it is necessary for me to give any comment on this case. The fact speaks for itself. Goh died barely two months after this aborted surgery. What do you think – would he have died earlier or later if he did not undergo that surgery?
This is one book which I believe everyone should read – Confession of a Medical Heretic by Robert Mendelsohn. The author is not an ordinary man. In the US, he wrote a syndicated column called “The People’s Doctor”. He was an associate professor at the University of Illinois Medical School and a director of Chicago’s Michael Reese Hospital. He was also chairman of the Medical Licensure Committee for the state of Illinois. In Chapter 3 of his book, Dr. Medelsohn wrote:
I believe that my generation of doctors will be remembered for … the millions of mutilations which are ceremoniously carried out every year in operating rooms.
Conservative estimates … say that about 2.4 million operations performed every year are unnecessary.
My feeling is that somewhere around ninety percent of surgery is a waste of time, energy, money and life.
Modern cancer surgery someday will be regarded with the same kind of horror that we now regard the use of leeches in George Washington’s time.
Greed plays a role in causing unnecessary surgery … there’s no doubt that if you eliminated all unnecessary surgery, most surgeons would go out of business.
Ignorance plays a part in a lot of unnecessary surgery.
Greed and ignorance aren’t the most important reasons why there is so much unnecessary surgery. It’s basically a problem of belief: doctors believe in surgery. There is a certain fascination in “going under the knife” … that (surgeon) can overcome anything because he can operate you … “You don’t have to take care of yourself, we can fix you if you go wrong.”
To protect yourself … your first step is to educate yourself. Get a second opinion. If you decide that surgery isn’t the answer, do whatever you have to do to detach yourself from the situation. In any situation short of an emergency, you’ve got plenty of time not only to decide whether or not you need the surgery but also who should perform the operation.
Wang (not real name, M872), 48-year-old male from Medan had been living with “blood-in-his-stools” for the past ten over years. This problem was attributed to piles. In November 2010 he came to a private hospital in Penang for a medical checkup. A scope of his colon did not show anything wrong. However, an ultrasound of his abdomen showed an ill defined, 7 x 9.2 cm mass in the right lobe of his liver.
Blood test was positive for Hepatitis B. Liver function test indicated elevated liver enzymes – ALT = 101, AST = 43 and GGT = 107. Alpha-fetoprotein was normal at 4.84.
CT scan done on 12 November 2010 indicated a 8.2 x 7.2 cm mass suggestive of hepatoma in segment 8 of his liver. A small solid lesion is also found in segment 7 measuring 1.8 x 1.2 cm. This may represent a satellite lesion of hepatoma. A simple cyst is noted at segment 8 below the right hemidiaphragm.
Wang went to see another doctor in another hospital. A repeat CT scan was done on 13 November 2010. The results were similar to the one done a day earlier.
The surgeon suggested that Wang undergo surgery to remove the tumour. The operation would cost RM 40,000. After the operation, Wang would have to undergo chemotherapy. The cost of each chemo is around RM 4,000 to RM 5,000.
Wang and his wife were disappointed and decided to go back to Medan without doing any surgery or chemotherapy. Someone learnt about their predicament and suggested that they come to CA Care for advice. We spent more than an hour with them. Below is a video recording of a part of our conversation that day.
Comments:
Most of the story-telling was done by Wang’s wife. She only talks Chinese! It appears to me that she is a “smart and wise” lady even though she is not educated.
She said: “When the doctor (surgeon) said that my husband had to undergo surgery and chemotherapy, I knew that this is a serious case”. This shows that she is not a dumb, naïve village girl – never mind if she does not know how to read the CT scan report or figure out what the blood test shows.
I asked her: “Did you ask the doctor if surgery can cure his cancer.” She replied yes. Most patients who come to us did not do that! How could that be? They don’t even want to find out what the prognosis is like! Not this lady.
She even asked the doctor: “What if we do not do the chemotherapy?”. The surgeon replied: “It is like cutting the lallang. You need to apply chemical after you mow it down. Only then can it be eliminated.” The answer was right on spot because this lady works in the farm – she understood it well. To kill off the lallang you need to apply chemical poison. Sometimes the land had to be dug up or overturned to get rid of the rhizome. So she said: “Then what would that do to my husband?” The implication is – what would happen to the patient if you poison him like you poison the lallang?
She also asked the surgeon: “When you cut up my husband, what are the chances that his cancer is cured?” Again this kind of question is never asked by most patients before they undergo an operation. The surgeon replied: “More than 80 percentage success rate.”
I asked the lady: “The doctor said 80 percent success – did you believe him?” She replied NO. I asked her why. She said: “There is one statement that the doctor made which got stuck in my head. Earlier I asked the doctor about the risk involved – how certain was he that everything would turn out right.” The doctor replied this lady: “The same case like you flying in from Medan to Penang. The airline does not guarantee that you are risk free.” Though the doctor did not admit outright that the treatment has risk, his reply very much implies that there is risk – the lady got the answer.
Later in our conversation, I came to know that Wang’s sister also had liver cancer. She received chemotherapy. She died after four cycles. While many patients or their loved ones appear naïve – don’t under estimate them! They have gone through some bitter experiences in life and they are not about ready to forget them. For such people, doctors need to do a lot of convincing to make them accept chemotherapy again.
I feel sorry for this couple. They came all the way to Penang and had to spend so much money. They can do the treatment – no problem about that for as long as they can pay the hospital bills – but cure appears to be elusive.
There is one important lesson we can learn from this story. How reliable or true are statements made by a doctor? Is it backed by good statistics and good research? At this point I am reminded of what some doctors wrote. Let me quote.
Dr. Block, herself a doctor, wrote in the foreword of Fight for Your Health: “Don’t just blindly follow what your doctors say. Find out the truth for yourself.”
Dr. Mendelsohn, in his book Confessions of a Medical Heretic wrote: “Doctors in general should be treated with about the same degree of trust as used car salesmen. Whatever your doctor says or recommends, you have to first consider how it will benefit him … because surgeon gets paid when he performs surgery on you, not when you’re treated some other way.”
Dr. Chestnut in his book, Lying With Authority wrote: “Somebody has got be lying – lying with an air of authority. The vast majority of surgery and drugs, including chemotherapy, does not treat or cure disease; it treats symptoms – often with devastating side effects.”
Dr. Hamilton in his book, The Scalpel and the Soul wrote: “As doctors, we generally don’t tell outright lies. We just don’t speak the truth fully.”
It is not nice to say that doctors tell lies – but the above quotations seem to say that some do, though they represent a minority. But I must say I like what Dr. Hamilton said: “We generally don’t tell outright lies. We just don’t speak the truth fully.” In this story, the surgeon told Wang and his wife that the treatment has more than 80 percent success.” His answer can be dead right or dead wrong! Let me explain.
From the perspective of this surgeon he is absolutely right to claim that the treatment has more than 80 percent success rate. A surgeon’s job is to cut up patients. After that he passes the patient to the oncologist or someone else. As far as he is concern his part of the cancer war is done. With the present state of the art technology, surgery carries minimal risk – like us flying in an air plane. The possibility of a crash is there but it is not likely (yes, it can happen!). Dying from surgery does occur although it is not likely.
But is that what the patient is looking for – just not dying from surgery? From the perspective of Wang and his wife, they are looking for a cure of his cancer! To them, the answer of 80 percent success takes an entirely different meaning. Cure means completely elimination of the cancer and it will not come back. That is what all patients ask for. Therefore, if patients are made to believe that they can attain an 80 percent chance of cure if they undergo surgery or chemotherapy is definitely false.
Let me repeat what Dr. Hamilton said: “we just don’t speak the truth fully.” Does this mean that doctors intentionally withhold some vital information which patients should know? If so, is that fair? I think the most vital information not told to patients is that though surgery is safe it will NOT cure the cancer. The chances of recurrence after an apparent successful surgery are very high. If you follow the case studies presented in this website, you will know that some patients die not long after their liver surgery.
Perhaps is this the reason why Dr. Mendelsohn said we should regard doctors in general “with about the same degree of trust as used car salesmen”?
In this article I have refrained from commenting if indeed the advice to operate is appropriate or otherwise. I would like to believe that the doctor has recommended this path with the best of intention. Even that, we need to be reminded that according to liver experts only 10 % to 30% of those who present with HCC are candidates for surgery. Meaning surgery is not the answer for all cases of liver cancer. Also surgery is good for only small tumours. Again, Dr. Mendelsohn’s words come to mind, they do this “because surgeon gets paid when he performs surgery on you”.
Let me conclude this article by trying to answer my earlier question: to what extent is the statement “after surgery there is a more than 80 percent success” true. I spent time reading my oncology books again. Below are the scientific facts written by liver experts. Read them carefully and come to your own conclusions.
Review of Medical Literature on Liver Cancer (Hepatocellular Carcinoma – HCC)
Research Reports
Ikeda et al., Cancer, 71:19-251993, reported: Eighty-three patients with HCC were treated with curative surgical resection during the past 8 years. No operative deaths occurred. Recurrence rates after resection at the ends of years 1, 2, and 3 were 37.0%, 57.1%, and 71.6%, respectively.
Iwatsuki et al., Ann Surg. 1991 September; 214(3): 221–229, reported: From 1980 to 1989, 76 patients with HCC underwent subtotal hepatic resection. Only 12 patients lived more than 5 years.
Vauthey, et al., American J of Surgery; Vol: 169, pg. 28-35, 1995, reported: Between 1970 and 1992, 106 patients underwent hepatic resection for HCC at Memorial Sloan-Kettering Cancer Center. Overall survival was 41% and 32% at 5 and 10 years, respectively.
Nagao et al., Ann Surg. 205(1): 33–40; 1987 reported: Ninety-four patients underwent hepatic resections from 1963 to 1985.One-, 3 and 5-year survival rates were 73%, 42% and 25% respectively. The recurrence of carcinoma was the main cause of death in 56% (42 patients) who died after discharge from the hospital. Prognostic factors that influenced the long-term prognosis were: preoperative alpha-fetoprotein level (less than or equal to 200 vs. greater than 200 ng/mL), tumor size (less than or equal to 5 vs. greater than 5 cm), and tumor capsule.
Shyh-Chuan Jwo, et al. Hepatology , Vol. 1367–1371; 1992 reported: A total of 238 patients who received curative hepatic resections during the last 10 years were observed. The results revealed that tumor size, tumor appearance and DNA ploidy were the factors in predicting tumor recurrence after resection for HCC. Patients with a tumor size less than or equal to 5 cm or a tumor appearance of the solitary type had better disease-free survival than did those with a tumor size greater than 5 cm or a tumor appearance of multiple/daughter nodule types.
Poon et al. of the Centre for the Study of Liver Disease, University of Hong Kong Medical Center, Queen Mary Hospital, Hong Kong,, Ann Surg. 234(1): 63–70 2001, wrote:
HCC is notorious for poor prognosis because of its invasiveness and frequent association with cirrhosis.
Hepatic resection remains the treatment of choice for HCC.
During the past decade, hepatic surgeons have focused much effort on improving the surgical techniques and perioperative management for resection of HCC, resulting in greatly improved perioperative outcomes. By the end of the 1990s, studies from our institution and others have demonstrated that a zero hospital or surgical death rate could be achieved in large series of patients.
Long-term prognosis after resection of HCC remains unsatisfactory. Disease-free survival has been poor because of a high incidence of recurrence. A 5-year cumulative recurrence rate of 80% to 100% has been reported.
Reports in the 1990s from Eastern and Western centers have documented a 5-year overall survival rate of 26% to 44% after resection of HCC.
Oncology Textbooks
Harrison’sPrinciples of Internal Medicine 15th Ed., pg.589.
Staging of HCC is based on tumour size, ascites (present or absent), bilirubin and albumin.
If untreated, most patients die within 3 to 6 months of diagnosis.
If detected very early, survival is 1 to 2 years after resection.
Surgical resection offers the only chance for cure, however, few patients have a resectable tumour at the time of presentation because of underlying cirrhosis or distant metastases.
Radomised trials have not shown a survival advantage after chemoembolization.
Liver cannot tolerate high doses of radiation.
The disease is not responsive to chemotherapy.
The American Cancer Society’s Clinical Oncology, 3rd Ed., pg. 399-401.
Only 15% to 30% of patients with HCC are candidates for surgery.
Conditions that render HCC unresectable are extensive disease within the organ itself and metastases.
Large tumour size, bilobar involvement and presence of cirrhosis do not necessary preclude resection but adversely affect mortality and prognosis.
Resection generally is limited to patients with small peripheral lesions and preserved hepatic function.
Five-year cure rate for all HCC who have undergone hepatic resection is approximately 30%.
The value of radiotherapy is limited in treating HCC.
Chemotherapy is palliative. Patients who respond to chemotherapy will survive 9 to 12 months longer.
Mean survival for patients receiving chemotherapy is approximately 5 months (1- year survival is 27%, 2-year is 8%).
Cure and long-term survival are possible only when tumours can be resected completely.
Martin Abeloff, et al. Clinical Oncology, Vol: 2, pg. 1697, 1703-1721.
Median survival of Hong Kong patients with inoperable HCC – tumour larger than 6 cm in diameter and receiving no treatment – was 3.5 weeks.
Tumour size at diagnosis is an important prognostic variable.
Tumour doubling time ranged from 1 to 19.5 months, with an average of 6.5 months.
Study in Japan showed that for patients with cirrhosis and HCC less than 3 cm in diameter and without treatment, 1-year survival rate was 90.7%; 2-year was 55.0%; and 3-year was 12.8%.
Unfortunately only 10 to 15% of newly diagnosed HCC patients are candidate for resection.
Presence of cirrhosis is a negative prognostic indicator.
Operative mortality rate of liver resections for HCC is les than 10%, but post-operative morbidity rate remains high – between 40 to 60%.
85% of hepatic recurrences develop within 2 years of resection.
There is little evidence of significant therapeutic activity for any single chemo-agent. There is also no evidence to support the routine use of combination chemotherapy.
Liver resection is the operation of choice for patients with tumors less than 5 cm in the absence of cirrhosis. In these patients, an operative mortality rate of less than 2% can be expected in experienced centers.Following liver resection, up to 75% of patients will develop intrahepatic recurrence within 5 years. Source: http://emedicine.medscape.com/article/197319-treatment
Sam is a 51-year old male from Indonesia. Sometime in May 2008, he had pains in his abdomen. A check up in a hospital in Sarawak indicated gall bladder stone. Sam underwent an operation to remove the stone. At the time of the surgery, the doctor discovered that Sam’s liver was not good. A CT scan revealed possibility of a hepatoma or liver tumour.
Sam was asked to undergo a liver operation in Singapore which would cost him about S$50,000.00. Sam came to Penang instead and underwent an operation for his liver in a private hospital. This cost him RM 35,000.00. This operation was done in October 2008.
CT Scan Report: 3 October 2008: There is ill-defined hypodense lesion at Segment VI. It measures 3.5 x 3.5 cm. Feature is suggestive of right lobe hepatoma.
Histology Report: 7 October 2008: Liver tissue weighing 350 gm, measuring 140 x 120 x 60 mm. Diagnosis: hepatocellular carcinoma.
After the surgery, Sam underwent two times of chemoembolization, in December 2008 and January 2009. Each treatment costs about RM 5,000.00.
In February 2009, Sam suffered severe jaundice. The blood test results on 10 February 2009 is a below.
Total bilirubin
523.77 H
Direct bilirubin
394.69 H
Alkaline phosphatase
143.34 H
GGT
758.75 H
ALT
121.38 H
AST
109.07 H
Alpha-fetoprotein
5,845.0 H
Sam underwent another surgery to install a metallic stent in the upper common bile duct. This procedure costs RM 20,000.00.
A CT scan done of 10 February 2009 indicated:
Worsening of the liver with increase in the number and size of the liver nodules.
There was thrombosis of the adjacent portal vein extending partially to the main portal vein.
In spite of such deterioration, nothing was done. And Sam was sent home without much explanation.
Sam and his wife came back to Penang again in March 2009. Unfortunately this time, the surgeon who operated on Sam’s liver was rather “hostile” in his attitude. It was a complete change of the surgeon’s attitude from the previous time before Sam had the operation. Sam and his wife felt let down and cheated. Sam’s wife said that before the operation the surgeon even hugged her and assured her that Sam would be alright. Now, after the relapse he did not even want to talk to them. They also told us that surgeon insisted that Sam undergo the surgery immediately because it was a very serious case. Sam and his wife requested go home and think it over first. The surgeon told them that if they returned to Indonesia, there would be a delay and by that time Sam’s condition would have deteriorated and he (the surgeon) would not be able to perform the surgery any more. Sam and his wife were virtually coerced into making their decision.
Listen to this video conversation.
Some excerpts:
Chris: You came to Penang – what did they say?
Sam: I had to be operated.
C: Before you did the operation, did you ask the doctor if surgery would cure you?
S: It must be removed.
Wife: Otherwise the cancer will increase more and more.
C: That is not true! Oh, you came here and they say cut and you agreed to get cut?
W: If we don’t operate, it is going to be dangerous. So, okay we agreed to the operation.
C: Let me ask you one more thing. Before you came here, before the operation – what was your condition? Were you healthy?
S: I was alright – healthy.
C: And after the operation, and having spent RM 35,000.00 – were you better?
S: No.
W: Before the operation, the surgeon was very friendly to us. He talked to us very nicely.
C: Oh, before the operation, Ibu (mama) asked anything and the doctor would answer you? He was nice to you?
W: Yes, he answered our questions and was very nice. But after the operation, he did not want to say anything anymore. We wanted to consult him but he did not want to talk to us. When we asked him questions, he just walked away. In a rush he just said – No problem, no problem and left us.
S: No, we were not able to talk to them like this (with you).
C: Before the operation, he talked to you nicely?
W: Yes, correct, correct. He even hugged me and assured me – Don’t worry, don’t’ worry, he (my husband)would be well and alright.
S: Oh, he was so sweet.
W: We felt so good and comforted. He told us the operation has to be done immediately.
S: It told him I was not prepared for it yet. The surgeon leaned back and sighed: Arr … if you don’t do it now, your condition will deteriorate.
W: He said: I would not be able to operate you anymore.
C: Wah, that is what he told you? If you go back to Pontianak first, your condition would get worse and you would probably be half dead?
W: By that time, it would be difficult to help.
C: That could not be true at all.
S: We did not have other alternative.
C: Yes, I fully understand. Patients are often rushed into making decisions. I don’t believe this is correct. Sometime, doing nothing is better than doing something.
The blood test results on 6 March 2009 are as below:
Total bilirubin
138.00 H
Direct
114.66 H
Alkaline phosphatase
143.34
GGT
203.05 H
ALT
57.98 H
AST
98.45 H
Alpha-fetoprotein
239,595.00 H
Sam then moved on to see another doctor who prescribed him two oral drugs. 1) Baraclude (entecevir) which is commonly prescribed for Hepatitis patients. 2) Nexavar – a drug that cost RM 20,000 per month. (Note: Pang in another story was also asked to take similar drug, which his doctor said was only 20 to 30% effective).
Sam took the drug, Nexavar for a day and a half (i.e., a total of 3 tablets). He suffered the following side effects:
He felt tired when walking or even talking.
His chest felt tight.
His ear started to produce a humming sound throughout the day.
His sleep was disturbed.
Sam and his wife came to seek our help on 8 March 2009 and decided to give up further medical treatment.
Comments:
This is a very tragic story indeed. Professor Jane Plant wrote: Conventional cancer treatment can process patients to the extent that they no longer understand what is really being done to them. It started with a threat or instill of fear in patients. Your liver is rotten – if you don’t get it out it is going to kill you. And you must do it fast! And look what has become of Sam now? Dr. Richard Fleming (in Stop inflammation now) wrote: … all forms of surgery cannot provide a long-term cure because they do not deal with the underlying cause of the disease, which is inflammation … Surgery often triggers an even greater inflammatory process, which encourages the illness.
Sam handed us the reading of his alpha-fetoprotein (AFP) below.
Study the above numbers carefully. Sam’s AFP value was only 3.0 before the gall bladder operation. After the operation, his AFP started to increase, from 50.5 to 3,201. Then he came to Penang and underwent a liver surgery. The situation got worse. As of March 2009, Sam’s AFP has exceeded a quarter million.
AFP (alpha-fetoprotein) Reading
19 December 2007
3.0
Done in Sarawak
7 May 2008
Gall bladder Operation in Sarawak
11 July 2008
50.5
Done in Sarawak
25 September 2008
2,433
Done in Sarawak
4 October 2008
3,201.97
6 October 2008
Liver operation in Penang
5 December 2008
18,550
Done in Penang
30 December 2008
17,857.8
Done in Penang
10 February 2009
5,845.0
Done in Penang
6 March 2009
239,595.0
Done in Penang
When Sam tried to seek clarification with the surgeon, he was snubbed. The surgeon did not even want to talk to Sam and his wife. Sadly, patients like Sam were left in a limbo. Sam was then passed on to another doctor.
Sam was prescribed an extremely expensive drug – at RM 20,000.00 per month. Of course, Sam had no choice. Accept it or die. But the point is: Was Sam told that the drug would not cure him? No, and he did not have the slightest clue about the truth. The data provided by the drug company’s website clearly indicated the following: For liver cancer,
Patients who took Nexavar – median survival = 10.7 months
Patients on placebo (sugar pill) – median survival = 7.9 months.
Nexavar only increased survival by 2.8 months. No where in the website does it ever say Nexavar cures liver cancer.
If ever there is anything we can learn from this story, it is this: Ignorance can kill. For years, we at CA Care, have been trying to empower patients by providing them with knowledge. However, patients are not interested to read or find things out for themselves. Far too often, patients prefer to find an easy way out and remain ignorant. And then when they reach this desperate end stage they would say to us: Oh, but we do not know all these. We trust the doctors.
Note: In mid-April 2009, we were informed that Sam died. Sam was operated on in October 2008 and by April 2009 he was dead. That was just six months after surgery.
What do you think has hastened his death?
Was it the surgery or his cancer?
What could have happened if Sam did not do anything?
Could he have lived much longer (minus the hefty hospital bills)?










You must be logged in to post a comment.