Can this statement be true? Is it a hoax? I would NOT dare say or write such a thing about chemotherapy lest I would be accused of trying to scare you away from chemotherapy – the gold standard treatment of cancer today. That is the way it is with human nature – if you say something not nice about something then you are the enemy of that something – there is no middle ground.
Unfortunately, my daily reading of medical literature makes it difficult for me to keep quiet or play deaf and dumb about what I have read.
When patients go and see their oncologists for their cancer, they generally have high hope but at the same time are just as anxious. Some patients dare ask their oncologists: Can chemo cure me? Others do not have a clue what to say or ask . They take it for granted that doctors know best – why ask questions? For those who asked, what answers do they get? Probably these: There is a 95 percent chance; or Let’s see after three cycles of chemo; or Cannot cure, but can control the cancer from spreading; or You must do chemo to make the cancer less aggressive, or With chemo you have better quality of life!
The answers provide much comfort and assurance to patients. Indeed that is what patients want to hear! And then they play along with their oncologists. But do you ever realize that such an answer is just a PR exercise rather than a statement of fact based on scientific evidence? With each passing day as more and more scientific evidence are being reported, such answers seem to be very leaky.
Let me ask you.
- If you know that chemo CANNOT cure your cancer, would you still undergo chemotherapy?
- If chemotherapy can make your cancer worse and makes it spread more aggressively, would you go for chemotherapy?
Some will say NO. But some will say YES, because what choice have I got? For example, read this e-mail below:
14 June 2012: Dear Chris,
The doctor (looked experienced and kind) suggested Gemzar and Cisplatin for six cycles. He did not recommend radio because it is not solving the root cause of the growth (previous radio sites also growing). Honestly, I’m at loss because I also frightened of chemo after so many awful stories. Finally, we decided to try out 1 or 2 cycles and monitor my husband’s condition, scheduled to start next week. I know this sounds stupid. However, there does not seem to be other avenue to slow down this growth. We still plan to continue with herbs long term- but can we have herbs during chemo? Thanks and regards.
30 January 2013: Dear Chris,
My husband had passed away last November 2012. After two cycles of chemo, he experienced leg weakness. He stopped chemo after that. Then he was paralysed starting from the legs, and moving upwards to both hands, and finally his breathing muscle was affected. He died due to breathing difficulties. In any case, I would like to thank you for the help rendered. Thanks and regards,
After two cycles of chemo and the patient was dead? This is what I always tell patients: It is your life and you have to make your own decision without me having to influence you. My responsibility is to provide honest information. You can ask your oncologists about the pros of chemo. But it is unlikely that they tell you in detail the cons of chemotherapy. Here, we tell you about the dark story of chemo because they are equally important although less talked about. Nevertheless you need to know them if you want to make a wise and empowered decision. But be reminded that by doing this we appear to be anti-chemo. We are not – at times we do urge you to go for chemotherapy.
Dr. Morton Walker (in Cancer’s Cause, Cancer’s Cure) wrote: I was astounded at how distorted the physicians’ presentations were when they discussed the side effects of their treatments. The doctors appeared to become almost like used-car salesmen in a pitch for their surgery, radiation therapy and/or chemotherapy. I know something about medical practices and oncology from my work as a medical researcher and as a former practicing podiatrist. In my opinion, the information the oncologists gave my fiancee was hardly an honest assessment of the relative benefits and risks associated with the recommended treatments.
Let me ask you to reflect on the following tragic story and see if you can learn anything from it.
Kathy (not real name) is a 44-year old lady. A CT scan done on 8 November 2010 showed a mass in her right lung. The doctor suspected malignancy, Stage 3B. A biopsy confirmed lung cancer, positive for EGFR (epidermal growth factor receptor), a case where taking oral drug, Iressa is said to be effective. Kathy started to take Iressa for seven months. With Iressa the mass in her lung started to shrink until the size could not be measured.
In August 2011, Kathy’s condition deteriorated. The lung mass which had apparently disappeared after taking Iressa, had grown back to twice its original size. Kathy was told that her lung cancer was at Stage 4B.
The lung mass was again tested for its sensitivity to Iressa. Unfortunately this time it was negative for EGFR. Iressa would be useless for Kathy this time around. Kathy was asked to undergo chemotherapy.
In November 2011, Kathy went to China for further medical treatment. Kathy underwent the following treatments:
1. Chemotherapy, a procedure called Transarterial Chemical Infusion (TACI).
2. Cryosurgery (also called cryoablation).
3. Radioactive iodine seed implantation.
Kathy was told that she had a 60:40 chance of success – 60 percent that she would be cured by the treatments and 40 percent chance that the treatments would fail.
Kathy made a last visit to China in March 2012. She was told she was unable to receive anymore chemotherapy because the tumour had grown in between her ribs.
Kathy was asked to take Iressa (again? But she had taken Iressa before from December 2010 to June 2011). Kathy declined Iressa.
Kathy was asked to return to China for a checkup in June 2012 but she did not return. She did a PET scan in Jakarta. Unfortunately the results showed progressive disease and the cancer had spread to her bones, lymph nodes, liver, etc.
This effectively means the treatments in China had failed.
Back home in Jakarta, Kathy continued to receive radiotherapy to her backbone. She also received chemotherapy. A CT scan in October 2012 showed that the tumour had grown in size. She stopped chemotherapy.
Unfortunately after the radiation to her backbone, her right breast became hard, painful and developed rashes.
Kathy had probably reached the end of the road and did not know what else to do. She said: Now I only take supplements and PRAY. Through a friend she got to know CA Care and came to Penang on 12 November 2012.
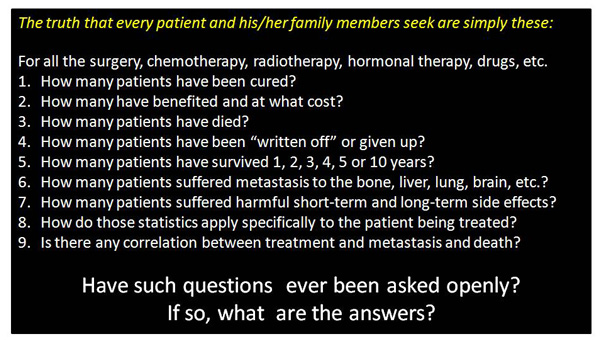
Ask the following questions:
- Iressa made the tumour disappear for a while – seven months. Does any cancer patient ever been told or know a complete story? Is there no evidence to show that shrinkage after treatment is just temporary and meaningless? If you have been reading our stories here, you know that there are many similar cases!
- Why did the cancer come back after its disappearance? Probably you will get the answer in the later part of this article.
- The lung tissue that was once positive for EGFR had then turned negative for EGFR – why? Is this not about the complexity, uncertainty and messiness of life that experts generally fail to see. Probably you will also get a scientific answer to this problem in the later part of this article.
- Kathy went for more treatments in China with the prospect that she would have a 60 percent chance of cure, in spite of the earlier failure. But it did not turn they way she or her doctor expected. She had MORE treatments and she ended up with MORE cancer.
- Can it be true that chemo and radiation encourage more cancer? Make the cancer more aggressive and spread more? Read further to know. It is up to you to make your own conclusion after that.
Research at the Fred Hutchinson Cancer Research Centre, Seattle, Washington, USA.
A research report, published in Nature Medicine 18: 1359-1368 (2012) has this title: Treatment-induced damage to the tumour microenvironment promotes prostate cancer therapy resistance through WNT 16B. It was written by Yu Sun et al. – a team of eight researchers led by Peter Nelson of the Division of Clinical Research, Fred Hutchinson Cancer Research. http://www.nature.com/nm/journal/v18/n9/full/nm.2890.html ) From this paper we learn that:
- Acquired resistance to anti-cancer treatment is a problem in cancer treatment.
- Cancer tissue microenvironments can influence the success or failure of treatments.
- WNT 16B in the prostate tumour microenvironment promoted tumour cell survival and disease progression.
Many articles are written in lay language following the release this study. This is to allow you and me understand the implications of the above scientific finding.
Read this article written by Jonathan Benson: Study accidentally exposes chemotherapy as fraud – tumors grow faster after chemo! (24 January 2012: http://www.naturalnews.com/038811_chemotherapy_tumor_growth_fraud.html#ixzz2JVhgUwC5)
The Daily News of 6 August 2012 had this heading, Shock study: Chemotherapy can backfire, make cancer worse by triggering tumor growth (http://www.nydailynews.com/life-style/health/shock-study-chemotherapy-backfire-cancer-worse-triggering-tumor-growth-article-1.1129897#ixzz2JiaJnOox)
Anthony Gucciardi wrote this article, Woops! Study Accidentally Finds Chemotherapy Makes Cancer Far Worse (7 August 2012, http://naturalsociety.com/chemotherapy-makes-cancer-far-worse/#ixzz2JibCe87N).
Let me summarise what these authors wrote.
- A team of researchers from Washington state had a giant Oops! moment recently when it accidentally uncovered the deadly truth about chemotherapy while investigating why prostate cancer cells are so difficult to eradicate using conventional treatment methods.
- Chemotherapy does not actually treat or cure cancer at all, but rather fuels the growth and spread of cancer cells, making them much harder to stamp out once chemotherapy has already been initiated.
Jonathan Benson said:
- You might call it the smoking gun that proves, once and for all, the complete fraud of the conventional cancer industry. Not only is chemotherapy, the standard method of cancer treatment today, a complete flop, based on the findings, but it is actually detrimental for patients with cancer.
- According to the study, chemotherapy induces healthy cells to release WNT 16B, a protein that helps promote cancer cell survival and growth.
- Chemotherapy also definitively damages the DNA of healthy cells.
- This combined action of healthy cell destruction and cancer cell promotion technically makes chemotherapy more of a cancer-causing protocol than a cancer-treatment protocol.
- Avoiding chemotherapy improves health outcomes. For all intents and purposes … the entire process of chemotherapy is completely worthless, and is actually highly detrimental for cancer patients. Anyone searching for a real cure will want to avoid chemotherapy, in other words, and pursue an alternate route.
Co-author Peter Nelson from the Fred Hutchinson Cancer Research Center explained:
- WNT 16B, when secreted, would interact with nearby tumor cells and cause them to grow, invade, and importantly, resist subsequent therapy.
- Completely unexpected – our results indicate that damage responses in benign cells … may directly contribute to enhanced tumor growth kinetics.
- In cancer treatment, tumors often respond well initially, followed by rapid re-growth and then resistance to further chemotherapy.
Deadly Cancer Drugs Make Cancer Worse and Kill Patients More Quickly
This finding should not come as a big shock really. Just before this discovery, medical researchers have also reported that certain cancer drugs not only fail to treat tumors, but actually make them far worse. The cancer drugs were found to make tumors spread and grow massively in size after consumption. As a result, the drugs killed the patients more quickly.
Vesseline Cooke et al. (and a team of 15 researchers headed by Raghu Kalluri of the Matrix Biology, Department of Medicine, Beth Israel Deaconess Medical Centre and Harvard Medical School, Boston, MA, USA, wrote an article: Pericyte Depletion Results in Hypoxia-Associated Epithelial-to-Mesenchymal Transition and Metastasis Mediated by Met Signaling Pathway. This was published in Cancer Cell . (http://ac.els-cdn.com/S1535610811004478/1-s2.0-S1535610811004478-main.pdf?_tid=dc206a6a-6d05-11e2-b7ac-00000aacb361&acdnat=1359788451_ea0e924ab8a26cdaa5bab696f3a0baf6)
- Researchers examined drugs such as imatanib (Gleevec, a leukemia drug) and sunitinib (Sutent, a drug for gastrointestinal tumors and kidney cancer) found that these drugs may initially reduce tumor size but afterwards cause tumors to spread aggressively – meaning the tumors can come back much stronger and grow much larger than their original size.
- In the study the researchers induced anti-angiogenesis in mice genetically engineered to have breast cancer. When they induced anti-angiogenesis, they saw a 30 percent decrease in the volume of each tumor over 25 days. But the number of tumors that had metastasized to the lungs tumors tripled compared to untreated control mice.
- Kalluri and his team performed a previous study in humans that found breast cancer patients with fewer cells called pericytes, which support the walls of veins, were less likely to survive their cancer. It turns out those are the cells damaged by some anti-angiogenesis drugs.
- By studying the mice they found that those pericytes are important because without them tumors become weak and leaky.
- And that causes cancer cells to launch survival mechanisms: the researchers found a fivefold increase in factors inside the pericyte-lacking cells that promote cell migration and growth.
In an article on 19 January 2012: Exposed: Deadly Cancer Drugs Make Cancer Worse and Kill Patients More Quickly http://naturalsociety.com/deadly-cancer-drugs-make-cancer-worse-and-kill-patients-more-quickly/#ixzz2JbbnsoG4 Anthony Gucciardi wrote:
- Cancer drugs, pushed by many drug companies as the only scientific method of combating cancer alongside chemotherapy, have been found to actually make cancer worse and kill patients more quickly.
- Sold at a premium price to cancer sufferers, it turns out these drugs are not only ineffective but highly dangerous.
Kristen Philipkoski, on 17 January 2012 (http://gizmodo.com/5876919/how-cancer-drugs-make-cancer-worse-and-kill-patients) wrote this article How Cancer Drugs Make Cancer Worse and Kill Patients.
- You’d think that a tumor shrinking would be considered good news for anyone suffering from cancer. But maybe not. Scientists have found that a type of cancer treatment aimed at shrinking tumors can actually make them spread more efficiently and aggressively and kill patients quicker.
I spoke to Dr. Raghu Kalluri, one of the study’s authors and chief of the matrix biology division at Beth Israel Deaconess Medical Center in Boston. He said:
- Focusing on tumor growth, the treatment results looked good. Tumors shrunk. But if you looked at the big picture, making tumors smaller didn’t mean the cancer was being controlled. It was actually spreading.
- Whatever manipulations we’re doing to tumors can inadvertently do something to increase the tumor numbers to become more metastatic, which is what kills patients at the end of the day.
I’ve had several family members who died at the hands of cancer shortly after the good news that doctors had shrunk the tumor! Was that tumor shrinkage actually what killed them?
Dr. Kalluri said:
- It’s possible. If cancer drugs are used randomly against all kinds of cancer without thinking about all the biology of the tumor, it could lead to a poor prognosis. It’s important for doctors to remember that tumors contain lots of types of cells, and they’re not all bad.
- Seventy to 80 percent of cells in a breast tumor are non-cancer cells. Are they all bad? Some of them are there to protect us.
- Cancer drugs that shrink tumours by cutting off their blood supply may end up helping them to spread.
- Drugs such as Glivec and Sutent reduce the size of tumours but could also make them more aggressive and mobile.
- A little-studied group of cells called pericytes that provide structural support to blood vessels act as gatekeepers to pen in cancer.
- Pericytes are wiped out by some advanced cancer drugs that prevent the growth of tumour-nourishing blood vessels. As a result tumours find it easier to spread around the body.
- Tests on mice showed that both Glivec and Sutent depleted pericytes by 70 per cent while metastasis rates tripled. They saw a 30 per cent decrease in tumour volumes over 25 days, but also a three-fold increase in the number of secondary tumours growing in the animals’ lungs.
Leon Watson, on 18 January 2012, wrote this article: Cancer drugs that aim to shrink tumours by cutting blood supply can actually help them SPREAD (http://www.dailymail.co.uk/health/article-2088032/Cancer-drugs-aim-shrink-tumours-cutting-blood-supply-actually-help-SPREAD.html#axzz2Jiz17J7D) explained further:
To see how relevant the findings were to patients, the scientists went on to examine 130 human breast cancer samples.
- Samples with low numbers of pericytes in tumour blood vessel networks correlated with the most deeply invasive cancers, distant cancer spread, and five and 10-year survival rates lower than 20 per cent.
Lead researcher Professor Raghu Kalluri, from Harvard Medical School in Boston said:
- But when you looked at the whole picture, inhibiting tumour vessels was not controlling cancer progression. The cancer was, in fact, spreading.
- Some assumptions about cancer must now be revisited. We must go back and audit the tumour and find out which cells play a protective role versus which cells promote growth and aggression. Not everything is black and white. There are some cells inside a tumour that are actually good in certain contexts.
S. L. Baker, 19 January 2012, wrote Breaking news: cancer drugs make tumors more aggressive and deadly (http://www.infowars.com/breaking-news-cancer-drugs-make-tumors-more-aggressive-and-deadly/)
- When natural health advocates warn against mainstream medicine’s arsenal of weapons used to fight cancer, including chemotherapy and radiation, their concerns often revolve around how these therapies can weaken and damage a person’s body in numerous ways.
- But scientists are finding other reasons to question some of these therapies. It turns out that while chemotherapies may kill or shrink tumors in the short term, they may actually be causing malignancies to grow more deadly in the long term.
- Scientists at the University of Alabama at Birmingham (UAB) Comprehensive Cancer Center and UAB Department of Chemistry are currently investigating the very real possibility that dead cancer cells left over after chemotherapy spark cancer to spread to other parts of the body (http://www.naturalnews.com/029042_cancer_cells_chemotherapy.html).
- And now comes the news that a little-explored specific cell type, the pericyte, found in what is called the microenvironment of a cancerous tumor actually may halt cancer progression and metastasis. And by destroying these cells, some anti-cancer therapies may inadvertently be making cancer more aggressive as well as likely to spread and kill.
These results are quite provocative and will influence clinical programs designed to target tumor angiogenesis, Ronald A. DePinho, president of the University of Texas MD Anderson Cancer Center, said in a press statement. These impressive studies will inform and refine potential therapeutic approaches for many cancers.
An article in http://www.bewellbuzz.com/body-buzz/chemotherapy/ has an article entitled Truth About Chemotherapy. It makes a good conclusion to our discussion.
- Chemotherapy drugs cannot differentiate between healthy cells and cancer cells, and attack both with the same vigor.
- Scientists have found that non-cancerous cells that were damaged by chemo drugs release a certain protein, WNT 16B, in high quantities. WNT 16B secreted by healthy cells damaged by chemo drugs interact with nearby cancer cells, increasing their survival rate and, more disturbingly, making them more resilient to other treatments.
- Studies show that chemotherapy drugs can cause DNA mutations. Scientists suspect that these DNA mutations may be passed to a patient’s future generations as well. In other words, chemotherapy drugs may negatively affect a patient’s entire hereditary line.
- Researchers at the Beth Israel Deaconess Medical Centre, Boston, studied the effect of cancer drugs and found that they caused cancer cells to metastasize aggressively.
- In their findings, scientists noted that cancer drugs, Sutent and Gleevec , caused cancer cells to metastasize. The size of the tumor may initially reduce when these drugs are administered. However, these drugs make cancer cells metastasize aggressively over time.
Is it time we look beyond chemotherapy? Maybe yes. More studies should be performed to better understand the role of natural substances in cancer treatment.
Recent studies show that cancer drugs are not only ineffective in treating cancer, but that they cause the tumor to metastasize aggressively, and, thus, decrease the lifespan of cancer patients. Also chemotherapy is astronomically expensive, leaving many patients or their families financially ruined while the drug companies continue to profit.
Do your research before you commit to being poisoned with chemotherapy.















You must be logged in to post a comment.