
At the end of our lives, what do we most wish for? For many, it’s simply comfort, respect, love.
BJ Miller is a palliative care physician at Zen Hospice Project. Listen to what he has to say.
Gist of what Dr Miller said:
- The American health care system has more than its fair share of dysfunction … I’m a physician … a hospice and palliative medicine doc, so I’ve seen care from both sides. And believe me: almost everyone who goes into healthcare really means well — truly. But we who work in it are also unwitting agents for a system that too often does not serve.
- Healthcare was designed with diseases, not people, at its center. Which is to say … it was badly designed. And nowhere are the effects of bad design more heartbreaking … than at the end of life.
- For most people, the scariest thing about death isn’t being dead, it’s dying, suffering.
- It can be very helpful to tease out suffering which is necessary as it is, from suffering we can change.
- The former is a natural, essential part of life, part of the deal, and to this we are called to make space, adjust, grow. It can be really good to realize forces larger than ourselves. They bring proportionality, like a cosmic right-sizing.
- After my limbs were gone, that loss, for example, became fact, fixed — necessarily part of my life, and I learned that I could no more reject this fact than reject myself. It took me a while, but I learned it eventually.
- Another great thing about necessary suffering is that it is the very thing that unites caregiver and care receiver — human beings. This, we are finally realizing, is where healing happens. Yes, compassion — suffering together.
- On the other hand, so much of the suffering is unnecessary, invented. It serves no good purpose. But the good news is, since this brand of suffering is made up … we can change it.
- How we die is indeed something we can affect. Making the system sensitive to this fundamental distinction between necessary and unnecessary suffering … our role as caregivers, as people who care, is to relieve suffering — not add to the pile.
- Palliative care — a very important field but poorly understood — it is not limited to end of life care. It is not limited to hospice. It’s simply about comfort and living well at any stage. So please know that you don’t have to be dying anytime soon to benefit from palliative care.
- So much of what we’re talking about today is a shift in perspective. Perspective … turning anguish into a flower.
- After my accident, when I went back to college, I changed my major to art history. Studying visual art, I figured I’d learn something about how to see — a really potent lesson for a kid who couldn’t change so much of what he was seeing.
- In my work over the years, I’ve known many people who were ready to go, ready to die. Not because they had found some final peace or transcendence, but because they were so repulsed by what their lives had become — in a word, cut off, or ugly.
- We know, from research what’s most important to people who are closer to death: comfort; feeling unburdened and unburdening to those they love; existential peace; and a sense of wonderment and spirituality.
- We need to … set our sights on well-being, so that life and health and healthcare can become about making life more wonderful, rather than just less horrible.
- I am asking that we make space — physical, psychic room, to allow life to play itself all the way out — aging and dying can become a process of crescendo through to the end. We can’t solve for death.
Comments
We are indeed fortunate to have a medical doctor to share his thoughts about death and dying. Many terminally ill cancer patients come to us hoping to find a “miracle” — hoping us to “cure” their cancer. Don’t be misled, we cannot cure your cancer! To make your life a bit better, may be. As Dr. Miller said, our role as caregivers, as people who care, is to relieve suffering — not add to the pile. Not to add more man-made misery to the unnecessary suffering.
We always tell patients who come to us:
Be committed to your healing, change your lifestyle and diet and take the herbs. Go home and find peace with your Creator. If you can eat, can sleep, can move about and have no pain — then be grateful for what you are. When it is time to go, “go home” in peace.
After hearing these words, gladly some patients fully agree with us. Perhaps, for some, the healing process starts if they realise and learn to “accept” the reality of the situation they are in.
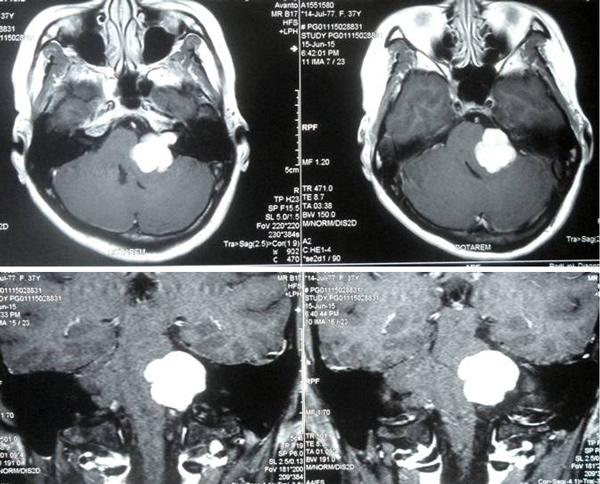
TN was a 65-year old lady with lung cancer that had spread to her bones and brain. She had 5 times radiation to her spine and ribs (end of October to early November 2013), 5 times radiation to her brain (January 2015) and another 5 times radiation to her spine, hip and brain in April 2015.
In addition she took Tarceva, starting 15 November 2013 and stopped in April 2015. The medication cost about RM 8,000 / month. She suffered dry skin and had a black spot on her nose after taking this medication (picture below).

The oncologist recommended chemotherapy since Tarceva was no longer effective. TN and her family decided not to go for chemotherapy as recommended by her oncologist. They came to seek our help in May 2015. She presented with constipation, breathlessness when walking, swelling of both legs and difficulty in sleeping (had to take sleeping pill). TN was prescribed some herbs and told to change her diet.
The following are two follow up e-mails from her daughter.
Dear Dr. Chris,
My mom has taken the capsules & herbal teas for a week. Briefly here is her condition:
- She has regained some strength – she can walk longer. Previously she felt breathless after 3 steps of walking.
- Appetite slightly improved. (Thanks to the variety of recipes from your wife’s cookbook)
- However she finds it difficult to speak more now due to shortness of breath. Her speech sometimes slur.
- Still unable sleep well at night, feel tightness/heaviness in the chest.
- No constipation – she passed motion after drinking the constipation tea for three days (3 times).
- Stomach & feet remain bloated and swollen.
I have brought my mom to see the oncologist. This is a follow up visit after the last radiotherapy session on 20 Apr. The current X-Ray report is unfavourable. She has a lot of fluid in her lung as compared to the previous X-ray. Oncologist recommended to flush out the fluid from the lung and this to be followed by pluerodesis. This is to give my mom some relief. I am quite concern of this and unsure if this will be beneficial to my mom.
Dear Dr. Chris,
My mother was discharged from hospital on Monday (25.5.15).
- The amount of fluids drained from her left lung is about 1.2 litres. The fluids were mixed with blood. We were informed by the doctor that was due to the bleeding from the tumour at her lung.
- In addition her left lung has also collapsed due to the fluids. Thus, she is still experiencing shortness of breath when she walks far.
- From the x-ray reports, it was found that some of the bones at the spine area have became brittle (osteoporosis). My mother was give 1 injection of XGEVA to relieve her pain.
Sadly, TN died not long after this. And this is the letter we received from her daughter.
Dear Dr. Chris,
My family and I would like to express our heartfelt thanks and appreciation for your kindness and efforts to help my beloved mother in her journey of cancer illness.
My beloved mother has passed away 2 weeks ago peacefully. I believe the herbal teas . medicinal herbs prescribed by your had helped a lot in making her illness less painful and rough.
Once again thank you for everything you did for my later beloved mother.
Best regards. Daughter of late Mdm TN.
Datukn Haji A was playing golf when he suddenly felt severe abdominal pain. Subsequent medical check-up showed cancer in the pancreas that had spread extensively to his liver. The doctor told him to go home… no surgery or chemotherapy. Not knowing what to do, Datuk and his family flew to seek our help. Datuk told us, “I understand. The doctor indirectly told me to go home and wait to die.” He presented with severe pains. Indeed his condition was beyond “help.” Anyway, we prescribed him some herbs – at least to lessen his suffering.
The following are some e-mails that his wife wrote:
Fri, Aug 7, 2015
Dear Prof,
My husband hs been in great pain at his tummy & lower back especially in the evening & night till 4a.m. this morning.
This morning he woke at 8a.m., pain reduced. Now after the superfood pain again. It relieves when taking gastrovit in warm water. Thank you.
Dear Prof,
My husband’s condition is better today. Less feeling of vomiting, less pain at his tummy & able to do more exercise. Thank you.
Dear prof,
He is in great pain now. since last night on off pain. Ok. If he can’t bear I’ll give him hospital’s pain killer. He said he will try to bear it till he can’t. He always feel good after gastrovit. Thanks Prof.
Dear prof,
Suddenly he feel much less painful. Can read newspapers. Will this pain subsides after 2 weeks?
Dear Prof,
Of course 2nd week better than 1st week physically (rashes on skin disappear, energy level better, no vomiting, etc.) except for the pain inside which we don’t know why?
1st week pain was at the tummy. now no more at tummy and had gone to the back and at the bowel area. The pain could be sharp at times. He said, this week energy is better than last week except for the pain.I hope it is not the cancer attacking. Good night.
Dear prof,
The pain is so great he can’t lie down to sleep. Terrible. Backache. So worry. Is this normal?
Good morning Prof,
Last night was better. This morning pinggang & bowel area not painful but lower abdomen (below pusat) pain & urine not good. Stomach & lower back skin dry. Still Hiccup. What to do? Thank you.
Dear Prof,
He is admitted to hospital. Kaki bengkak & not able to urine (now fix a tube to drain out) & sakit at pinggang & lower tummy. Stomach bloated. Doc injected pethidine.
Yes Prof. His condition not good.
Thank you.
Sep 6, 2015 at 5:30 AM
Dear Prof & wife,
My husband passed away peacefully on 4th Sept 2015 @ 3.30am. Thank you for everything. The herbs help me a lot at this difficult time. No more discomfort at the tummy area. Thank you.
Let us end this article by highlighting a report in the mass media. Take time to reflect on this.
Survey shows nearly half Malaysian cancer patients go broke a year after diagnosed
A survey was done in eight Southeast Asian countries, and in Malaysia, had followed 1,662 cancer patients in public and private hospitals through their first year following diagnosis, with 44 per cent of them at 50 years old or younger.
The Asean Costs in Oncology (Action) study by Sydney-based George Institute for Global Health made the following conclusions:
- 44 per cent of respondents would survive the cancer with no financial catastrophe, while another 11 per cent died.
- Around 51 per cent will be pushed into “economic hardship” after a year from diagnosis, with 49 per cent of them already used up all their personal savings, while 39 per cent of all respondents could not pay for their medication.
- Of the respondents, 35 per cent could not pay for medical consultation fees, 22 per cent could no longer pay for their rents and mortgages, while 19 per cent of them just discontinued treatments altogether.
- “The cost of cancer does not only affect patients, but also their families and society as a whole,” the institute’s Prof Mark Woodward said.
- The survey found that the median age where Malaysians are diagnosed with cancer is at 52 years, and subsequently died at 59.
- “Cancer diagnosis at stage III or IV (late stage) makes treatment more costly, less likely to succeed, and reduces chances of survival.”
- It also found that patients become financially vulnerable from two reasons: high out-of-pocket spending on loans, debts and depletion of assets; and high treatment and medical spending.
- The Action report said even patients in public hospitals face high out-of-pocket spending for many health services such as chemotherapy, biopsy, biomarker testing, innovative cancer treatments, and palliative care.
- UM’s cancer epidemiologist Prof Dr Nirmala Bhoo-Pathy said the average cost for breast cancer treatment could reach up to US$15,000 (RM65,000) per year, and those earning less than US$1,100 (RM4,700) per month would have “a very difficult time” to pay for it.
Read more Are Medical Bills Killing Patients?https://cancercaremalaysia.com/2013/04/11/are-medical-bills-killing-patients/
Question to ask: How do you want your life to end? Leave a hole in the family’s bank account? Many patients from Indonesia had to sell their houses or land before they died. You have a choice!
















You must be logged in to post a comment.