You have to take care of your diet! If you want to eat anything you like, there is no need to come and see me! Useless, waste your time and my time!

You have to take care of your diet! If you want to eat anything you like, there is no need to come and see me! Useless, waste your time and my time!
Review by Yeong Sek Yee & Khadijah Shaari
At the 3rd Malaysian International Conference on Holistic Healing for Cancer organized by Cansurvive Centre Malaysia (www.cansurvive.org.my) in October 2013, we met an Australian lady who introduced us to the above book written by an Australian cancer survivor, Barry Thomson. The book, for some strange reason is only available from the publisher in Queensland or from the author (www.defeatcancertwice.com).
In April 2003, Barry Thomson, a businessman, was diagnosed with two primary concurrent melanomas. This meant that he had two separate deadly melanomas, each with the potential to spread and develop secondary melanoma. Basically, this doubled his chances of dying from melanoma cancer. His own family doctor twice advised his wife to “sell your business and do anything that you have ever wanted to do.” Clearly he believed that his two melanomas would prove to be terminal. His only chance to beat melanoma was to find his own cure or he would surely die.
Barry was also told by a leading oncologist, that no treatment was available as chemotherapy and radiation are ineffective against melanoma. Barry was grateful to this HONEST oncologist who made him realize that he had to seek healing utilizing natural therapies.
Barry admits that, in 2003 he had (and still have) no medical background or training as he started a frantic search for information that would show him how to use natural therapies to become free of melanoma. His own extensive research, plus information from numerous books by cancer survivors and others, enabled him to compile a cancer fighting regimen which helped him to defeat his melanomas.
This resulted in his first book, “Join Our Escape from Death Row-Cancer Jail” which was publish in late 2007. (Website: www.cancerjailescape.com).
In June 2008, Barry had to battle terminal cancer for a second time. He was diagnosed with bowel cancer (also known as colon cancer) which totally blocked his large bowel. He underwent successful surgery to remove the tumour but, due to twists in the small bowel preventing intake of food, he underwent a second emergency surgery twelve days later. Extremely ill, he spent four nights in Intensive Care and was lucky to survive. He spent a total of 33 nights in hospital.
In March 2009, Barry had a third major surgery to rebuild his stomach and repair an incisional hernia and abdominal muscle separation. Subsequently, Dr. Matthew Carmody, his surgeon, told him that “100% definitely” he had cancer cells in his lymph system. He strongly recommended six months of chemotherapy for a “27% better chance of beating the cancer.” Barry declined and decided to use his experience in overcoming his melanomas in 2003 to eliminate the bowel cancer cells.
Colonoscopies in May 2010 and July 2012 showed NO POLYPS and NO CANCER. In July 2012 Dr. Carmody told Barry “Forget bowel cancer. You have certainly beaten it. See me again in six years for the sole purpose of checking for polyps with a colonoscopy.” It is now more than five years since his original diagnosis of bowel cancer.
After defeating melanoma and bowel cancer, Barry continued his research to find more and more effective natural cancer attackers. He gained a wealth of new and superb cancer-fighting information. In 2010, he felt it would be appropriate to write a second book to share this additional knowledge he had acquired with people fighting cancer.
It is not the intention of this review to discuss all the natural healing methods that Barry Thomson used to heal his melanomas and bowel cancer except to mention that some of the modalities that he used included hyperthermia, the Gerson therapy, Cantron, the Dr Johanna Budwig Cancer protocol, hydrogen peroxide, Cansema for skin cancer and proper nutrition. The book also lists other natural healing methods that Barry has researched and found useful such as far-infrared saunas, herbal teas, probiotics, juicing, wheatgrass and other sprouts, getting rid of parasites, etc
We do not intend to discuss the merits or demerits of Barry’s healing methods except suffice to mention that when one is diagnosed with cancer (any form of cancer), one has a wide choice of healing methods. The usual so –called “scientifically tested” protocols of chemotherapy and radiation, etc is just one of the many methods to heal cancer. You certainly do have choices just like Barry Thomson and many others.
Do read and investigate further first before you jump into the bandwagon (of conventional cancer treatments). As Barry said…”the true facts of the situation are that, while still in total shock over their cancer diagnosis, patients are very quickly rushed into chemotherapy and/or radiation treatments”
If you would like to read/research further on the other healing modalities for cancer other than chemotherapy and/or radiotherapy or together with chemotherapy and radiotherapy, we recommend that you check out the following books:
1) AN ALTERNATIVE MEDICINE GUIDE TO CANCER by Dr John Diamond, MD and Dr Lee Cowden, MD with Burton Goldberg. This is a very comprehensive text which tells that cancer can be reversed using clinically proven Complementary and Alternative therapies. NB: The authors also wrote CANCER DIAGNOSIS: WHAT TO DO NEXT which explains clinically proven, safe and nontoxic treatments.
2) THE DEFINITIVE GUIDE TO CANCER by Lise Alschuler, ND, FABNO and Karolyn A. Gazella…..An Integrative Approach to Prevention, Treatment , and Healing.
3) FIGHTING CANCER– A NONTOXIC APPROACH TO TREATMENT by Dr Robert Gorter, MD, PhD and Erik Pepper, PhD
4) CANCER THERAPY by Ralph Moss, PhD…The Independent Consumer’s Guide to Nontoxic Treatment.
5) OUTSMART YOUR CANCER by Tanya Harter Pierce…Alternative Non-Toxic Treatments That Work.
6) KNOCKOUT by Suzanne Somers…Interviews with Doctors Who are Curing Cancer.
7) LIFE OVER CANCER by Dr Keith Block, MD…read about the Block Center Program for Integrative Cancer Treatment
8) DEFEAT CANCER by Connie Strasheim…15 Doctors of Integrative and Naturopathic Medicine Tell You How.
9) COMPLEMENTARY AND INTERGRATIVE MEDICINE IN CANCER CARE AND PREVENTION by Dr Marc Micozzi, MD, PhD…Foundations and Evidence-Based Interventions.
10) INTEGRATIVE ONCOLOGY by Dr Donald Abrams and Andrew Weil
11) ALTERNATIVE TREATMENT FOR CANCER by Ping–Chung Leung and Harry Fong…Annals of Traditional Chinese Medicine Vol. 3
12) HERBAL MEDICINE, HEALING AND CANCER by Donald R. Yance…A Comprehensive Program for Prevention and Treatment.
13) MANAGEMENT OF CANCER WITH CHINESE MEDICINE by Li Peiwan
14) INTEGRATING CONVENTIONAL AND CHINESE MEDICINE IN CANCER CARE A CLINICAL GUIDE by Tai Lahans
15) SUPPORTIVE CANCER CARE WITH CHINESE MEDICINE by William C.S.Cho.
There are a lot more books and websites on complementary/integrative cancer treatments but doctors will invariably brush this aside as “quackery,” “unproven, unscientific,” etc. and they will definitely not recommend you to read them.
If you have been diagnosed with cancer and standing at a big T-junction and not knowing whether to turn left or right, we recommend that you read the following two new books by Dr Chris Teo, the founder of The Ca Care Therapy…visit www.cacare.com
CANCER: IS THERE ANOTHER OPTION?
CANCER: WHAT NOW?
Both books will give you an idea of a holistic, herbal option that you may not know about.
To conclude, let us tell you a very little known fact. When President Ronald Reagan was diagnosed with colon cancer in 1985 whilst still in office, he had surgery in the US but he did not opt for chemotherapy/radiotherapy. Instead he opted for some German “unscientific” therapy….read the story at the following link:
https://cancercaremalaysia.com/2014/01/29/how-ronald-reagan-healed-his-colon-cancer
Remember, you do have choices.

by Yeong Sek Yee & Khadijah Shaari
Shortly after he turned 70, Mr. Ralph De Angelo, a retired department–store manager in the heart of black America, saw a newspaper advertisement that claimed that prostate cancer screening saves lives. The advertisement also mentioned that 95% of men diagnosed with localized disease are cured.
The following is the tragic story of Mr. De Angelo after his prostate screening and how unnecessary harm can be done to those who go for screening of the prostate, breast, etc. This is a classic example of collateral damage (due to overtreatment) described in the book “HOW WE DO HARM” by Dr Otis Webb Brawley, MD a medical oncologist and Executive Vice President of the American Cancer Society.
In 2005, Mr. De Angelo, after his prostate screening, was diagnosed with prostate cancer, with a PSA reading of 4.3 ng/ml (just 0.3 above what is considered normal). He was urged to have a biopsy. Two of the 12 biopsies show cancer. The Gleason score was 3 plus 3 which is associated with the most commonly diagnosed and most commonly treated form of prostate cancer. There is no way to know whether a patient with this diagnosis will develop metastatic disease or live a normal life unaffected by the disease.
With this uncertainty, Mr. De Angelo was persuaded by his urologist to perform a radical robotic prostatectomy which he (the urologist) thought was the gold standard of care. After the operation, he was told he had a small tumour 5mm by 5mm x 6mm in a moderate size (50cc) prostate. The tumour was all in the right side of the prostate. This means that the tumor didn’t appear highly aggressive under the microscope. Good news? Unfortunately, Ralph realizes that he is now incontinent. Three months later, the incontinence is still there and he has to wear pampers continuously. Besides incontinence, Ralph was also impotent and given Viagra.
With a lingering 0.95 ng/ml (even though his prostate has been removed), a radiation oncologist suggested “salvage radiation therapy” to the pelvis. Four weeks into the radiation, Ralph saw blood in his stool. This was due to radiation proctitis i.e. radiation damage to the rectum. He continued having incontinence, but also developed a burning sensation upon urination. Later, Mr. De Angelo stopped his radiation with one more week to go. For the rectal proctitis, he went to a gastroenterologist, who prescribed steroids in rectal foam that he had to put up his rectum four times a day.
About three weeks after stopping the radiation, Mr. De Angelo realised that whenever he passed gas, some of it comes out of his urethra. He also sensed liquid from his rectum soiling his diapers. He was confirmed having a rectal fistula into the bladder…there is a hole between Ralph’s rectum and his bladder. After several urinary infections and when the fistula didn’t seem to be healing, he had to see a GI surgeon. He performed a colostomy to keep stool off the inflamed rectum and the hole into the bladder. The next step was an ureterostomy, a surgery that will bring urine to the abdominal wall and collect it in a bag, just like his bowel movements.
In Dec 2009, Mr. De Angelo’s daughter called Dr Brawley to inform him that her father had “urinary tract infection” which later progressed to sepsis, a widespread bacterial infection in the blood. On the fifth day of hospitalisation, Ralph passed away (only 4 years from diagnosis). Interestingly…”the death certificate reads that death was caused by a urinary tract infection. It doesn’t mention that the urinary tract infection was due to his prostate-cancer treatment and a radiation-induced fistula….Mr. De Angelo’s death will not be considered a death due to prostate cancer, even though his death was caused by the cure.
In conclusion, Dr Brawley strongly believed that… “the majority of these men, who are treated with radiation or hormones or both, got no benefit from treatment. They get only the side effects (collateral damage) including those that Mr. De Angelo had: proctitis i.e. inflammation and bleeding from the rectum, cystitis, burning sensation on urination and a feeling of urgency, a rectal fistula in which bowels and bladder are connected. The side effects of hormones can be diabetes, cardiac diseases, osteoporosis, and muscle loss.
In the case of Mr. Ralph De Angelo, both the surgeon and the radiation oncologist got paid handsomely. They both likely thought they were doing the right thing. However, Ralph got the side effects, and his quality of life was destroyed (too much collateral damage?).
One parting remark by Dr Otis Webb Brawley which is very relevant to this article:
“Prostate-cancer screening and aggressive treatment may save lives, but it definitely sells adult diapers.”
FOOTNOTE:
On the Malaysian scene, Malaysia’s leading oncologist, Dr Albert Lim passed away on March 8, 2013 due to prostate cancer which had spread to the bones and liver (and possibly lungs as well?) in just less than a year after diagnosis.
Was it overtreatment or was it excessive collateral damage?
Please share with us.
• Diagnosed with breast cancer
• Undergone mastectomy, costing Rupiah 30 plus million.
• Doctor asked to do chemo – I refused.
• My mother had ovarian cancer, Stage 3B. She had surgery and chemothrapy.
• Prior chemotherapy, she was well.
• After chemo cancer recurred, lumps grow again.
• Doctor recommended surgery and chemo again.
• Mother was too weak and declined medical treatment.
• She died within a year.
After an X-ray and CT scan, the doctor found a 7 cm tumour in my lung. It was a Stage 2 cancer. I refused to have a biopsy because I don’t want to undergo chemotherapy. I prefer to take herbs.
Why don’t you want to go for chemo?
No, no, it is not successful.
How do you know?
I have many friends – chemo, chemo, and 6 months later die!
One of my friend had lung cancer and he went for treatment in Singapore. He had to sell 2 houses to pay for the medical bills. He had chemo and chemo. Before 2 years were up, he was dead. Each chemo cost a few thousand dollars. He died and property also gone!
This book is written by Dr. B. M. Hegde. He is a visiting professor of Cardiology, the Middlesex Hospital Medical School, University of London; Affiliate Professor of Human Health, Northern Colorado University, retired Vice Chancellor, MAHE University, Manipal.
In the Foreword of the book, Professor Rustum Roy of the Pennsylvania State University wrote:
In this book Dr. Hegde expressed his thoughts very clearly and bluntly. Here are some of what he wrote:
Introduction
Man and His Problems
Integrity of Medicine
On Doctoring
Medicine and Money Making
Medical Philosophy
First, do no harm
Medical Consultation
Limits of Science
Medicine, Drug Studies & Statistics
Progress & Knowledge
Resistance to Change
Comments
With much respect, it is very hard to become a medical doctor, let alone become a “good” doctor. This is what it takes to be trained as a doctor in the US (in When doctors don’t listen by Leana Wen & Joshua Kosowsky).
Medical training in the United States is a long and prescribed process. Since all medical schools require a bachelor’s degree future doctors must first complete four years of undergraduate work at a college or university (this is called premedical).
The Results of this Extensive Medical Training? Cookbook Medicine, according to Drs Wen & Kosowsky,

Is this why Dr. Medelsohn made some hard comments below?
Robert Medelsohn, chairman of Medical Licensure Committee, State of Illinois, USA; associate professor at University of Illinois Medical School and director, Michael Reese Hospital, Chicago (in: Confessions of a medical heretic) said:

Medicine is Broken
Dr. Ben Goldacre (in Bad Pharma) came to a sad conclusion:

Medicine is Devoid of Theory and Concept of Health and Healing
Andrew Weil, graduate of Harvard Medical School and director, Integrative Medicine Program, University of Arizona in Tucson, Arizona, USA (in: Health & Healing) wrote:
by Yeong Sek Yee & Khadijah Shaari
Yes, the rich and famous (and insured) do die faster when they have cancer…more from the collateral damage due to the conventional (and scientifically proven?) cancer treatments than from the original cancer itself. A classic example is the sad story of Mrs. Jacqueline Kennedy Onassis who was diagnosed with Non-Hodgkin’s Lymphoma in January 1994 and died in May 1994, just barely 5 months after diagnosis.
In the best-seller, HOW WE DO HARM, Dr Otis Brawley, an oncologist and Vice-President of the American Cancer Society, bluntly stated that….”If you are rich and insured, you face another menace. Ironically wealth can increase your risk of getting lousy care. When wealthy patients demand irrational care, it’s not hard to find a doctor willing to provide it. If you have more money, doctors tell you more of what they sell, and they just might kill you. “
Below is a list of 15 (there are many, many more) rich and famous personalities who have succumbed to cancer and the average period from the date of diagnosis to death is less than 2 years. How is it that the scientifically proven/tested conventional cancer treatments did not help them? Did their cancer treatments come along with excessive collateral damage to their body system or were their cancers just too aggressive?
Likewise, you may remember that Malaysia’s most famous and leading oncologist, the late Dr Albert Lim, succumbed to prostate cancer on March 8th 2013 after less than a year of scientifically tested cancer treatments. He had metastasis to his pelvic area, liver and lungs as well. Was there excessive collateral damage or was the prostate cancer too aggressive??
HERE ARE THE 15 RICH AND FAMOUS WHO TRIED BUT DID NOT SURVIVE:
1) JO ANN DAVIS, 57
Jo Ann was a US Republican Congresswoman for Virginia and was diagnosed with breast cancer in 2005. She underwent chemotherapy treatments and a mastectomy. In early 2007, she suffered a recurrence. When the cancer returned, she underwent chemotherapy again. Jo Ann died on Oct 6, 2007.
Summary Point—From diagnosis to death: 2 years
2) LINDA McCARTNEY, 56
Linda McCartney, wife of Paul McCartney died in April 1998, less than three years after it was announced that she was treated for breast cancer. Although her chemotherapy treatments had seemed to have her cancer in check, she took a turn for the worse in March 1998 when the disease spread to her liver.
Summary Point—From diagnosis to death: Less than 3 years
3) HEATHER CLARKE, 39
Heather was the wife of Darren Clarke, a PGA Golfer. She died in August 2006 after a two year battle with breast cancer that had spread to her bones and liver. She was treated at the Royal Marsden Hospital in London.
Summary Point—From diagnosis to death: 2 years
4) MIRIAM ENGELBERG, 48
Miriam, a well-known US cartoonist was diagnosed with breast cancer in 2001 at the age of 43. Three years later, the cancer had spread to her brain and she died at age 48.
Summary Points—a) From diagnosis to recurrence: 3 years b) From diagnosis to death: 5 years
5) ELIZABETH EDWARDS, 57
Elizabeth Edwards, wife of John Edwards (a US presidential candidate) was initially diagnosed with breast cancer in 2004 and was treated with a combination of chemotherapy, surgery and radiation. In March 2007, a recurrence was discovered after she cracked a rib and a subsequent X-ray showed spots on another rib, on the other side of the chest.
Summary Point—From diagnosis to bone metastasis: Less than 3 years.
6) KING HUSSEIN OF JORDAN, 63
In July 1998, King Hussein was diagnosed with non-Hodgkin’s Lymphoma (NHL) and immediately underwent chemotherapy at MAYO Clinic in US. He was treated there for six months and returned to Jordan in January 1999.
In late January 1999, King Hussein returned to MAYO after his doctors found evidence that the lymphatic cancer had recurred. King Hussein underwent two bone marrow transplants with cells from his younger brother and sister (in December 1998 and January 1999).
In February 1999, King Hussein returned to Jordan for palliative care and subsequently passed away on February 7, 1999.
Summary Points—a) From diagnosis to recurrence: 6 months b) From diagnosis to death: 7 months.
7) FREDDY FENDER, 69
Freddy Fender, singer of hits like “Before the Next Teardrop Falls” and “Wasted Days and Wasted Nights” was diagnosed with lung cancer (two lemon-sized tumors) in January 2006. He underwent chemotherapy but later decided to stop treatment because of severe effects on his body. Following Fender’s initial round of chemo, he had a PET scan which showed that the tumors had shrunk, but also revealed that he had nine other tumors. Freddy Fender died on October 14 2006.
Summary Point—From diagnosis to death: 9 months.
8) SUZANNE PLESHETTE
On August 11, 2006, Suzanne Pleshette was treated for lung cancer at Cedars-Sinai Medical Centre and the hospital claimed that the cancer was the size of “a grain of sand” when it was found during a routine x-ray, that the cancer was “caught very much in time,” that she was receiving chemotherapy as an outpatient. She was later hospitalized for a pulmonary infection and developed pneumonia, causing her to be hospitalized for an extended period ……as part of her treatment, a part of her lungs was removed… Pleshette died in January 19, 2009of respiratory failure.
Summary Point—From diagnosis to death: 1 year 5 months
9) DAN FOGELBERG, 56
Dan Fogelberg, a singer and songwriter, discovered he had advanced prostate cancer in 2004. He underwent hormonal therapy and achieved a partial remission but failed to completely eliminate the disease. Dan subsequently died on December 15, 2007.
Summary Point—From diagnosis to death: 3 years
10) LUCIANO PAVAROTTI, 71
Pavarotti, opera singer was diagnosed with pancreatic cancer in July 2006 and required emergency surgery to remove the tumor. On September 5, 2007, Italy’s AGI news agency reported that Luciano Pavarotti’s health had deteriorated and the singer was in a “very serious condition”. He was reported to be in and out of consciousness multiple times, suffering kidney failure. He finally passed away on September 6, 2007.
Summary Points—From diagnosis to death: 11 months
11) DANA REEVE, 44
Dana Reeve, wife of Christopher Reeve (Superman), was diagnosed with lung cancer in August 2005 and passed away on March 6, 2006.
Summary Point—From diagnosis to death: 7 months only
12) TONY SNOW, 51
Tony Snow, a White House spokesman, was treated for colon cancer in 2005 at which time his colon was removed and subsequently underwent six months of chemotherapy. In March 2007, doctors determined that the cancer had spread to his liver. He died in July 2008.
Summary Points: a) From surgery/chemotherapy to liver metastasis: 1 ½ years b) From surgery /chemotherapy to death: 2 ½ years
13) MICHAEL LANDON, 54
Michael Landon was the star in the hit series “Little House on the Prairie” and “Bonanza”. On April 5, 1991 he was diagnosed with inoperable pancreatic cancer that had spread to his liver and lymph nodes. He underwent three sessions of chemotherapy but subsequently died on July 1, 1991.
Summary Point—From diagnosis to death: 2 months
14) ARCHBISHOP CHRISTO DOULOS, 69
The Archbishop fell ill in June 9, 2006 and medical tests showed that he suffered from advanced cancer in the LARGE INTESTINE (COLON) and an unrelated malignant growth in the liver. A first operation to remove the intestinal cancer was deemed successful but later a liver transplant in the US was abandoned after discovery that the liver cancer has spread. The Archbishop passed away in January 2008.
Summary Point—From diagnosis to death: 1 ½ years
15) MARTIN D. ABELOFF, 65
Dr Martin Abeloff, an international authority on the treatment of breast cancer and chief oncologist and director of the Sidney Kimmel Comprehensive Cancer Centre at John Hopkins University for the past 15 years, died of leukemia on September 14 2007. His leukemia, a form that is sometimes slow to grow, was diagnosed a year before that (i.e. approx September 2006).
Summary Point—From diagnosis to death: 1 year
In his book, Dr Otis Brawley revealed a secret: Wealth in America (and elsewhere as well) is no protection from getting lousy care…in fact, wealth can increase your risk of getting lousy care.
Do you fancy getting some collateral damage?
by Yeong Sek Yee & Khadijah Shaari
In this segment on collateral damage, we have decided to feature the late Datuk Ilani Isahak, the Chairman of the Interfaith Relations Working Committee until her passing away on February 24th 2011 after a 3-year battle against breast cancer. On June 12th 2011, Dr Amir Farid Isahak (Datuk Ilani’s brother) recounts his sister’s struggle in an article in The Star entitled “MY SISTER’S CANCER.” Our story below is essentially excerpted/adapted from Dr Amir’s article.
In Dr Amir’s own words, this is his story:
“THIS is not just another sad cancer story, but the story of the struggles my own sister, Ilani Isahak went through, fighting her breast cancer for three years until she succumbed to the disease in February this year (2011). She followed everything the oncologist prescribed. Each time, after discussing with me, she would decide “no more chemo”, but after the next visit with the oncologist, she would tell me “the oncologist said it is absolutely necessary that I go for the chemo, so I agreed”.
Soon after the initial six courses of chemo and one year of a “smart” drug ended, the cancer came back. The extremely expensive “smart” drug she was given was trastuzumab (Herceptin), which is a monoclonal antibody that targets the HER2 receptors on the breast cancer cells. However, a re-examination of her cancer cells then showed that she was not a good candidate for trastuzumab. The first report had been inaccurate.
So her oncologist put her again on further chemotherapy. Other drugs were then tried, and there was some response, but internally the cancer was encroaching into her rib cage and onto the lining of the lungs (pleura). Besides hair loss, her fingernails were blackened after the repeated chemo sessions.
The other “smart” drug she was given included bevacizumab (Avastin), which is also a monoclonal antibody that is supposed to prevent new blood vessel formation (anti-angiogenesis), thus preventing new cancer growth. (However, back in July 2010, the US FDA had evidence that bevacizumab was not suitable for breast cancer. In December 2010, the US FDA officially revoked its approval for the use of bevacizumab for breast cancer, saying that it is neither safe nor effective in breast cancer patients. The available data shows that bevacizumab neither prolonged overall survival nor slowed disease progression sufficiently to outweigh the risk it presents to breast cancer patients).
Until the last six months of her life, my sister was relatively well, which means she had about two years of reasonably “good quality” life. Then she started to have chronic coughs.
At first, she still managed to do her normal chores, but she gradually deteriorated, and became breathless easily. A pleural effusion (fluid in the space covering the lungs) was diagnosed, but the first attempt to drain the fluid failed to relieve her symptoms.
Exactly one month before her death, she had to be admitted to the hospital, and had permanent drainage tubes inserted into both sides of the rib cage, and she required the oxygen mask continuously. The doctors also decided that she could have palliative care only, with no further active treatment. After one whole month of suffering, she died.
My sister died because the cancer spread to a vital organ – her lungs. There was copious pleural effusion that repeated and even continuous drainage could not solve it. The effusion meant that her lungs gradually collapsed.
With the reduced oxygen supply, the heart had to work harder, and soon it also succumbed. Although there were discussions to attempt surgery to seal the pleural cavity (thus preventing the formation of the effusion), by that time, her poor general condition made any major surgery unsafe.
At her death bed, she told me “learn from my mistake, do not go for chemo”.
One of the major lessons about conventional cancer treatment that Dr Amir Farid imparted in his article is that:
“If the cancer patient is not cured after the first course of chemo, she is unlikely to be cured at all. Cancer cells which are resistant to the first chemo are most likely resistant to further chemo. Although each subsequent chemo may drastically reduce the number of cancer cells, the tough resistant ones will multiply and manifest their presence soon enough.”
NB: Dr Amir Farid Isahak is a medical specialist who practises holistic, aesthetic and anti-ageing medicine. He is a qigong master and founder of SuperQigong.
ACKNOWLEDGEMENTS:
The article was excerpted from the sources below which we acknowledge with thanks:
1) Breast Cancer: Ilani’s Message – Learn from my mistake, do not go for chemo
Link: https://cancercaremalaysia.com/2011/03/11/435/
Link: http://www.thestar.com.my/story.aspx?file=%2f2011%2f6%2f12%2fhealth%2f8879117&sec=health
Link: http://www.thestar.com.my/story.aspx?file=%2f2011%2f3%2f13%2flifefocus%2f8183426&sec=lifefocus
A lady school teacher came to see us in early 2012. Her husband is a medical doctor (later, I got to know that her daughter is also a medical doctor). She did not come with any medical report – she just wanted to tell me her story and based on that prescribe her herbs.
She had colon cancer that had spread to her liver. She had completed her chemo and had also undergone a RFA treatment (radiofrequency ablation). In spite of that, her CEA was rising.
The first question I asked her, “What do you want me to do? What do you expect to get when you come and see me?” Her answer, “I want to find a cure.” To that I told her, “No, I am sorry I don’t have anything to cure anybody. My herbs are not magic.”
Then I asked her to read my two books, Cancer – Why They Live and What You Need to Know About Chemos … She would not even look at the books! But she insisted on wanting to try my herbs. My answer was, “No. For now, I would not prescribe you any herbs. Go home and pray to your god (s) after you have gone through my websites – www.cacare.com and www.CancerCareMalaysia.com ”
Were we being cruel to send her home without giving her the herbs? Sometimes we need to be “apparently” cruel to be kind and honest. While we fully understand that patients who come to us are helpless, desperate and lost – it is extremely unfair and wrong for us to make them believe that we can offer them a cure for their cancers. Our experience over the past 18 years dealing with cancer patients tells us this fact clearly – No one on earth can cure cancer! You just have to learn to live with your cancer and heal yourself. Saying that the treatment gives you a response does not mean a cure. To achieve a tumour shrinkage after treatment is equally meaningless. Shrinkage generally does not translate into a cure. And saying that if you remain alive for 5 years means your cancer is cured is scientifically baseless.
These are the “truths” that you may have missed out or you have not been told. Read the medical literature, no one ever talks about cure for cancer. If they do, they generally mean being alive for 5 years. That is not cure! It is only a remission. We have seen cancer recurring even long after that. My aunty had a recurrence after 13 years. Her cancer spread to her lungs and she died.
So when we sent this lady teacher home to “learn” more we were just being truthful – we cannot cure any cancer. Unfortunately she did not want to learn. She portrayed as a well-informed patient who knew all the medical terms — “after all I am the wife /also mother, of medical doctors.”
Patients who come to us with this kind of “shopping-for-magic-bullet” mentality, are sure to be very disappointed with us. We would send them home without any herbs and ask them to think over.
We understand most patients who come to us are generally medically given up – they have gone though all possible medical treatments and failed. They have nowhere else to turn to for help. I used to jokingly tell patients, “Yes, we are the last one stop.” Given that situation what do patients expect us to do? Cure their cancers? And we, at CA Care, promising them a cure? Don’t be misled – we cannot cure your cancer. We also do not cure your medical results. At CA Care we want to heal you as a person. Healing is different from cure. Healing happens at all levels – physical, mental and spiritual.
Fast forward, April 2014 – about 2 years later. This same lady teacher came to see us again. I could not recongise her. She was dark (due to too much chemo?). I asked for her medical reports. Again – like before – she did not bring any. And she started to rattle her story below.
P: I was diagnosed with colon cancer in September 2010. I had an operation followed by 8 cycles of chemotherapy. I was okay for about 6 months. After that the tumour marker (CEA) started to go up. The cancer had gone to the liver. I did one time RFA (radiofrequency ablation). After one month, it seemed to be okay but my CEA did not go down. It was still climbing.
I did a PET scan and the result showed 2 tiny lymph nodes (collar bone) was infected, but the liver was okay.
I was started on chemo again – another 8 cycles. The CEA went down. It seemed to be okay. While on chemo, I was also given Avastin. After the chemo was completed, I was still on Avastin as maintenance.
A bit less than 6 months later, I did a PET scan. The doctor said everything was okay. But after the PET scan, the CEA started to go up again.
About a month later, I did a CT scan. There were tiny nodules in my lungs.
The oncologist started me on chemo again. This was the third round and I had 12 cycles. I was also given Erbitux.
After 12 cycles of chemo my CEA went down to 1.7 (normal 5). I continued to receive Erbitux as maintenance.
A scan later showed the nodules in the lung were still there but there were no other additional metastasis.
In October 2013, my CEA started to go up again. It was like 1.9.
My oncologist sent me to see a surgeon, to see if the infected lymph nodes could be removed. But the surgeon asked me to do a PET scan first before considering surgery. I did a PET scan. The result showed everything was clear except for one nodule in my right lung. This could be an early metastasis. The surgeon was unable to proceed with the surgery because the nodule was too small. So nothing was done.
Today my CEA started to go up again. And all this while I was still on Erbitux.
Just before the Chinese New Year (January 2014) the oncologist started me on 5-FU (chemo again). My CEA was going up and Erbitux was not effective anymore. That was why the doctor added the 5-FU. I received this every week.
Even with the added 5-FU my CEA had gone up to 5 (from 1.7 before October 2013).
I have been going for the chemo but for a few times now, I started to feel restless 5 or 10 minutes after receiving the drug. I felt restless and did not know where to put my legs, where to put my hands. I could not concentrate. When I talk to you, my eyes cannot focus on you. I am just restless and don’t know what to do. I don’t know whether this is the effects of the drug or it is psychological effect.
Two weeks ago, when they put the drug in, I felt very difficult. They called the doctor in. The doctor wanted to give me steroid (prednisone). But the week before I have asked the oncologist to take off the prednisone because it made me very drowsy. So when they wanted to give this again, I said no!
Last week I went to see my oncologist again. He stopped the Erbitux and said I was already too long on this. So he just gave me only 5-Fu. But I still felt restless even with only 5-FU.
In total I am on chemotherapy for three and half years. (Note: 3 rounds of chemo with a total of 28 cycles besides the weekly 5-FU, maintenance Avastin and Erbitux).
Chris: To be honest, I am surprised that you are still alive today. I really don’t know what I can do to help you. What do you expect me to do in this situation? Because I don’t believe that by taking the herbs your CEA is going to come down, honestly. Now it is just at 5.
Patient: But I am scared that it will go up.
C: Why do you worry wanting to get the CEA down – CEA is not going to kill you.
P: But every time the CEA went up, I went for a scan and they found something in there.
C: That is normal. We all know that. Nobody can cure any cancer. That’s my experience. What is more, even when you get cancer, they tell you to eat anything you like.
P: But I did “pantang” (abstain from certain food).
C: But the way you “pantang” is not the way we teach you to “pantang” at CA Care. It is useless if you don’t do it right. Follow what I tell you fully or don’t. No half measure. Again let me tell you. If you come and see me hoping that your CEA can come down, no, I don’t think that is the correct logic. Honestly, I don’t think it will come down. For three and a half years the doctors could not get it down, and you expect me to do it!
P: It will not come down but I hope it will not go up.
C: I don’t know. You need to know that cancer cells are not the same, they are different. After round and round of chemo, some cancer cells are killed, but some can still remain alive or are not affected by the chemo drugs. Because of that some patients suffer from “more aggressive” cancer after chemo. Researchers have shown that chemo makes cancer more aggressive. That is why chemo does not work.
This is the attitude of patients. When all else have failed they come to us and expect me to do magic. How could I do it? My answer to you is, I am not going to be able to do it – as simple as that.
Other people may say, “Yes take this and take that, your CEA will go down, etc., and etc.” But I am not sure if this is going to be true or not. Why don’t you come back to see us only after you have decided you don’t want to do anymore chemo?
P: I thought of stopping the chemo.
C: It is not a matter of thinking you want to stop chemo. You have to decide – do you still want to continue with your chemo. If you want to continue, go ahead with the medical treatment. You have to be clear about this. I suggest that you go home and continue with your chemo.
Come and see me only after you have decided to give up chemo totally. When you reach that point, and you don’t want to do chemo anymore, and you have nowhere to go, then come and see me. Then we will try the herbs.
For now, don’t take the herbs yet. Go back and when you tell yourself. “I don’t want any more chemo and I have nowhere else to go,” then come and see Chris Teo. Then I’ll give you the herbs.
P: Now, I want to take a break from chemo and I want to take the herbs.
C: Take the herbs for how long?
P: Your wife suggested to try the herbs for one month.
C: You can take the herbs for one month, but I am going to tell you it is not going to give you any significant effects. No way. You have been on medical treatment for three and a half years and it never worked and you can’t expect to take the herbs for a month and it is going to work!
P: Not to go down but to see if it can control it or what.
C: Let me tell you again. When doctors have failed to help you for three and a half years, how can you expect my herbs to help you in a month. No way.
P: But Dr. Teo, I have a friend in Kuala Lumpur. He has lung cancer. The doctor said he only has 3 months to live. He did not go for medical treatment and he took your herbs instead. He is still alive today. It has been one year already.
C: Of course, patients who have not gone for chemo do better with our herbs!
I am obliged to prescribe this patient some herbs. She came back to collect the herbs the next day. She asked my wife:
a) What are the side effects of the herbs?
b) What are these herbs?
c) Some herbs could be dangerous and affect the kidney, etc.
My wife replied: No one has died because of our herbs. And many have been taking these for years. If you are afraid of the side effects or think they are dangerous, please don’t take them!
Comments: For those who have cancer and who know how to read, I strongly suggest that you read my recent book, Cancer – What Now?
 In this book I have discussed many topics that are important to you and your survival. Going for whatever treatment for your cancer is about you and your choice. Your life is in your hands. When you get cancer, it is also about you. YOU, the person. It is not just about the tumour or the rising CEA, etc., etc.
In this book I have discussed many topics that are important to you and your survival. Going for whatever treatment for your cancer is about you and your choice. Your life is in your hands. When you get cancer, it is also about you. YOU, the person. It is not just about the tumour or the rising CEA, etc., etc.
I have written many articles trying to let you all know that shrinkage of tumour and decreasing of CEA are often meaningless. It makes you feel good for a few months and the cancer comes back again. Is this not what happened to the lady teacher above? PET scan said okay, all clear but soon something pop up again somewhere! More chemo again. When do you stop chemo?
In Chapter 3 of the book I talked about the types of patients who come to see us and their attitudes – wanting to find a magic cure when there is NONE. Of course, you can go for chemo, surgery, take this supplements and that supplements – beware of the empty promise! In Chapter 6, I wrote about the virtue of doing nothing!
I am aware that my way of dealing with cancer is rather non-conventional and against the commonly accepted norms. If you are following my writing in the websites, you will know that what we do in CA Care do help many patients. It is just whether you want to believe or not!
Look out for another story after this one. This is about a man with colon cancer who was at the point of death in the hospital and was asked to do chemo! His wife preferred to do nothing and brought him home in an ambulance! Like the Chinese say, if you have to die, die at home! This man remained alive at the point of time when I am writing this article.
SS (E345) is a 55-yer-old lady. Her problem started around October 2013 when she started to have coughs with a bit of phlegm. There was no blood. She consulted a GP who gave medication but the problem persisted on and off. At last she requested her GP to do an X-ray of her chest. There was “something” in her lung. SS was referred to a hospital in her hometown for a CT scan.
CT scan done on 18 October 2013 showed a lobulated mass at the right hilar region. It measures 2.9 x 3.2 cm. SS was asked to consult a lung expert in a private hospital in Penang.
Bronchoscopy and Surgery Failed
SS did a bronchoscopy. In this procedure the doctor inserts a bronchoscope into the nose or mouth. This allows him to view the inside of the airways and lungs. Unfortunately for SS, the bronchoscope could not penetrate the passageway deep enough and the doctor saw nothing! Fluid taken from the lung during the procedure did not show presence of malignant cells.
The doctor suggested a better option would be to do an open surgery. SS agreed but she was asked to do a PET scan first. The PET scan results on 30 October 2013 showed:
Based on the PET scan results the doctor was optimistic that surgery would provide good “success.” SS proceed with the surgery as recommended by the doctor. Unfortunately it was an open-close job – failed. The doctor took some tissue samples for biopsy.
The result of the biopsy indicated:
The tissue is positive for EGFR (meaning oral drugs such Iressa or Tarceva is indicated).
Consultation with Oncologist
SS was referred to the in-house oncologist for further management. The following are excerpts of our conversation.
Daughter: The oncologist said it is better to take oral medication than undergoing chemotherapy (infusion). Chemo has more bad side effects. My mother can take either Iressa or Tarceva.
Chris: Did you take the drug?
D: No. I asked the oncologist the following questions:
a) Are there side effects of the oral drug. His answer: Yes, patients may become itchy and have pimples or sores.
b) Can the oral drug cure my mother? His answer: Cannot cure. It is just to control.
c) Control for how long? His answer: It all depends on the patients.
d) From your experience, how long does the control last? His answer: For some patients the control lasted for one year. After one year, the drug was not effective anymore. But for some other patients the control lasted for 2 years before becoming ineffective.
e) After Iressa becomes ineffective, what do we do next? His answer: Go for chemotherapy (injection).
D: The cost of Iressa is more than RM 200 per tablet. It comes to about RM 8,000 per month. Why take it when it is not going to be effective?
C: After 1 or 2 years on the drug, you will then have to go for chemo. Did you ask if chemo is going to cure your mother?
D: No, chemo cannot cure her. Each chemo costs about RM 2,000 per cycle. Later cycles would cost more – RM4,000 to RM5,000. She needs to do 4 to 6 cycles first and then we will see what happen after that.
Reluctant Q & A Session at RM 100
C: When you ask such questions, did you see if the oncologist was happy to answer you?
D: He seemed very reluctant and uneasy. Appeared like he had the answer and he did not have the answer. Also appeared like wanting to answer and not wanting to answer.
C: How long was your consultation?
D: About an hour and his consultation cost RM 100.
C: Wow, that’s great! One hour! I am indeed very surprised that he gave you so much time. You as patient, need to ask and ask the doctor such questions before undergoing any treatment. Be empowered and don’t be dumb. Now, go home and read this comic book::

(See https://cancercaremalaysia.com/2014/04/14/info-about-lung-cancer-ignorance-kills/)
I have written many books but many people find reading difficult. Some people don’t want to read. Now, I make comic books instead so that you don’t have to read too much. You can finish reading this book within an hour. So go home and read this. Learn from the stories of these people. Be empowered – be smart. Example, if you take Iressa and this cost you RM 8,000 per month. So, for a year, that would come to about RM 90,000. But can it cure you? No! In addition you have to suffer from itchiness, etc.
Opted for Chemo at Government Hospital
C: Your head – bald? Why?
D: She had chemo at the government hospital in January 2014. She completed 4 cycles – each cycle at 3 weeks interval.
C: Did you suffer?
Patient: Not very bad. I was constipated. My head and some parts of my body became itchy.
C: Did you have to pay for the chemo?
D: Yes, RM 50 per cycle. They used Gemcitabine (Gemzar) + Cisplatin. After the fourth cycle, the CT scan showed stable result.
C: Okay, at least you did it at the GH and did not have to pay so much. If you were to do it at a private hospital, it could cost you anywhere from RM 4,000 to RM5,000 per cycle. (Note: For comparison, a patient from Indonesia has 12 cycles of chemo (same drugs – Gemcitabine + Cisplatin) in a private hospital in Singapore. The total bill came to RM 0.5 million. And the treatment also failed. See: https://cancercaremalaysia.com/2014/04/24/two-billion-rupiah-chemo-and-surgery-failed-oncologist-said-more-chemo-you-just-have-to-trust-me/ ).
Do more chemo, and more chemo – until you die?
Patient: The tumour did not grow bigger. It did not get small either.
D: The doctor said my mother had to take Iressa or Tarceva as a follow up. I again asked how long must my mother need to be on this oral drug. The answer: It all depends on the patient. When Iressa becomes ineffective, she will go for chemo again. So we decided not to take the drug.
C: It seems that you are going round and round the same road.
D: You do the chemo. Then you take oral medication. Then go for chemo again. Then take oral drug again.
C: Did you ask when can you stop the treatment?
D: No, no idea.
C: Oh, see how long can you stand the treatment? Then until you die?
D: Exactly.
C: So they are being honest with you. You need to know that there is no cure for lung cancer – even with chemo!
Take Home Lessons From This Case
1. There is no cure of lung cancer. The oncologist acknowledged that.
2. But of course, there is treatment (provided you have the money to pay for it, or are willing to endure the side effects).
3. According to the oncologist, take oral drug – Iressa or Tarceva. You will suffer less side effects.
4. Iressa or Tarceva does not cure. It may cost you RM 8,000 per month. And it may be effective for one or 2 years only.
5. When you have reached the dead end with oral drug, go for i/v (injection) chemo which also cannot cure.
6. Then, if you are still alive and still have the money to spend, go for oral drug again.
Have plenty of money to splurge?
You have an option to go to Singapore — go to the best and the famous. There they may also give the same stuff, chemo with Gemcitabine (Gamzar) + Cisplatin. That seems to be the gold standard.
A patient from Indonesia paid about RM 500,000 (half a million ringgit!) for 12 cycles of that stuff. Result: miserable failure. https://cancercaremalaysia.com/2014/04/24/two-billion-rupiah-chemo-and-surgery-failed-patient-said-ill-die-not-because-of-my-cancer-its-because-of-the-chemo/
Another Indonesian, was treated with one oral drug after another interspersed with chemo, over a period of about 3 years. He spent about half a million ringgit as well. Result: just the same failure and the cancer got worse. https://cancercaremalaysia.com/2013/11/29/lung-cancer-chemo-experiments-that-failed-and-failed/
Yet another Indonesia had chemo after chemo and spent about one million Singapore dollars and he died after about 2 years of treatment.
I have learned something interesting from this case study. If you wish to try your luck with chemotherapy but do not have the money to splurge, you still have a chance! Go to the (Malaysian) government hospital. This patient (SS) paid only RM 50 for a cycle of chemo with Gemcitabine + Cisplatin. For 4 cycles she only paid RM 200 — compared to half a million ringgit in Singapore! After all they use the same toxic drugs anyway! And the result is just the same, FAILURE – wherever you go!
If you want to opt for less hefty medical bills, then go local. Only that you don’t get to become the patient of the best and the famous. The husband of one lung cancer told me he spent about RM 300,000 over 2 years on his wife’s treatment. HIs wife took Iressa and had chemo after chemo. She died just after her husband came to see us.
Part 1: Two Billion Rupiah, Chemo And Surgery Failed:. Oncologist said, “More chemo, you just have to trust me!”
Chris: After 12 cycles of chemo had failed the oncologist said you have to keep on trusting him and you were asked to go for more chemo, and you spent 1.5 billion rupiah. What happened after that?
Son: My father nearly died. He could not eat. His body weight was down to 55 kg from 75 kg.
C: Before the chemo, how was his condition?
He was normal but now everything is not right with him. And these are his problems.

1. Both hands and legs – pins and needles / tingling. Very severe and is the main concern.
2. Legs – weak, no strength.
3. Can’t walk far – becomes breathless.
4. Sudden hot and cold – fevers.
5. Headaches.
6. Gastric problems and bloated stomach.
7. Feels heaty inside.
8. No appetite.
C: After the 12 cycles of chemo, did you go for more chemo (as advised by the oncologist)?
No, no more chemo.
C: Did you go and see another doctor?
No. My father said, “I’ll die not because of my cancer. It’s because of the chemo.”
Part 2: Two Billion Rupiah, Chemo And Surgery Failed: Patient said, ” I’ll die not because of my cancer. It is because of the chemo.”
This is an e-mail I received from Alex.
Selamat malam Dr Chris: Saya Alex dari Jakarta. Saya mau minta tolong Dr Chris untuk mengobati papa saya yang kena kanker paru dan setelah kemo dan operasi, kanker tersebut malah tumbuh di liver dan limpa. Saya rencana besok hari minggu, 20 April 2014 berangkat dari Jakarta ke Penang untuk konsultasi dengan Dr Chris … Saya mohon Dr Chris mengobati papa saya. Terima kasih banyak Dr Chris. Salam.
(Good evening Dr. Chris. I’m Alex from Jakarta. I wish to ask Dr. Chris to help treat my father who had lung cancer. After chemo and operation, the cancer spread to his liver and lymph. I plan to fly from Jakarta to Penang for consultation on 20 April 2014. I request Dr. Chris treat my father. Thank you.)
The next day, Alex came to our centre in Penang and related the tragic story of his father’s cancer treatment in Singapore.
Before that, I asked him, “Who asked you to come here?” Apparently after 2 years of treatment and spending about 2 billion rupiah (RM 600,000?) Alex’s father ended up with more cancer and suffered badly form the side effects of the treatment. Desperate and lost,someone in Sydney told Alex about a Chris Teo in Penang. He immediately googled “Cris Teo Penang” and found CA Care. He then bought a plane ticket and flew here the next day!
Indeed it is dramatic but this showed us his concern for his father’s health. Alex came with almost a bagful (his luggage) of medical reports and PET scans. This is his story (all in italic).
I come for my father, he is 62 years old. Yes, I bring all the medical reports and PET scans.
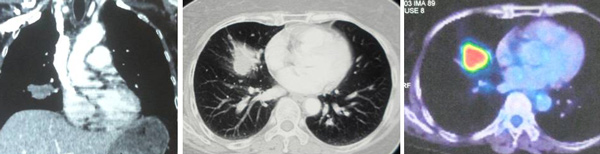
The problem started in March 2012. He went for a routine check up for his heart in Singapore. The CT scan showed a mass in his lung. PET scan was done followed by a biopsy. It was cancer. The tumour was about 3 cm and it had already spread to the lymph nodes.

CT scan report dated 21 March 2012: Presence of a 3.9 cm spiculated soft tissue density mass in the right lower lobe. A 0.9 cm right hilar lymph node is noted. The liver is normal with no focal nodules.
PET scan report dated: 18 April 1012: Bronchogenic malignancy, 3.5 x 2.6 cm. FDG avid right infra-hilar adenopathy.
The doctor suggested surgery but my father declined. However, he agreed to undergo chemotherapy. This was started in May 2012. He received a total of 12 cycles. Each cycle consisted of 2 injections. Each cycle started with an injection on day 1 and day 7. Rest for 14 days and then started with the next cycle.
Chris: Did you know what drugs they used on him?
??? Not sure! (later, the son found out that his father was given: Chemo drugs: Gemzar and Cisplain. Others: Zometa for the bone, Eprex (epoetin A) and Gran – blood boosters).
C: Why did you want to do chemo? Don’t you know that chemo is not good?
We didn’t know that. The only thing I know was that the effects were bad. But the oncologist told us: “If you were a member of my family, I would also ask you to do chemo.”
C: Did you fully believe what he told you?
Yes. But with time I learned from the internet chemo does not cure!
C: Did you ever ask the doctor if chemo is going to cure?
Yes, I did ask him. The oncologist said, ” We need to try first. There would be 30 percent chance of cure, the remaining 70 percent cannot be cured!
C: Which means that you only have a 30 percent chance of success and he asked you to try? Is that reasonable?
After 3 cycles of chemo, the oncologist said my father belonged to the 30 percent success group – can be cured!
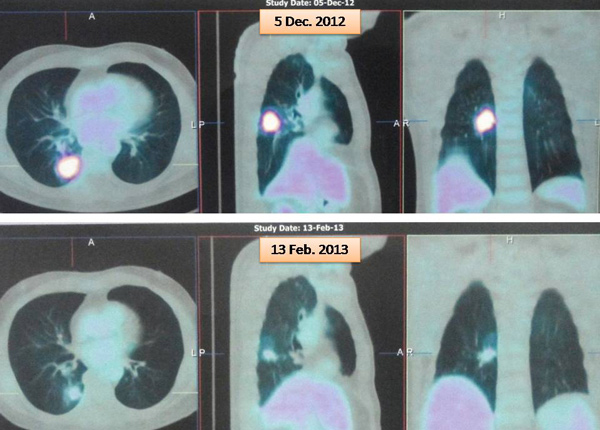
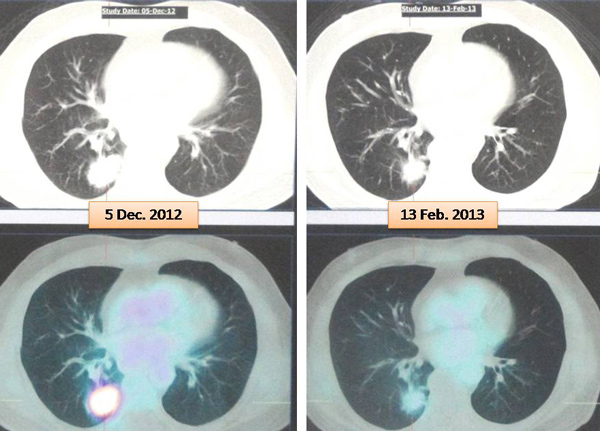
Study the above. The initial reaction to chemotherapy was significant shrinkage of tumour (but if you know enough this is just an illusion. It may not last – meaningless)
PET scan report on 13 February 2013: Reduction in uptake and size of the mass in the lower lobe of the right lung. Prior size 2.3 x 1.6 cm to 3.8 x 2.6 cm.
C: So you continued with the chemo?
Yes, until 12 cycles. But there was no cure.
C: Did you ask the doctor why earlier on he said you belonged to the 30 percent can-cure group but now he had failed to cure your father? What was his reaction to that?
He said, “You just need to trust me.”
So he asked you to trust him – what does that mean and what could this lead to?
He said, “Do more chemo.”
By then, did you still trust him?
(Shaking his hands negatively).
C: Only after 12 cycles of chemo – only then you realised that you could not trust him anymore? And did you continue with more chemo?


Study the above and you will note that more chemo does not make any difference now!
PET scan report on 8 October 2013: The previously noted hypermetabolic right lower lobe pulmonary mass appears to be larger. Current size 6.5x 4.2 cm versus prior size of 5.2 x 3.6 cm. There is interval development of a subcentimeter mildly FDG avid lymph node posterior and inferior to the right main bronchus.
From April 2013 (i.e. one year after diagnosis) until October 2013, my father did not receive any treatment. On 9 October 2013, he underwent an operation to remove the tumour in his lung. After the surgery he was not on any medication. On 14 April 2014, my father did a PET scan and there was no recurrence in his lung, but PET scan showed the cancer had spread to his liver and lymph nodes.

PET scan report 14 April 2014: Multiple FDG avid lesions in the liver – segments 7 and 8 (size of 6.5 x 3.6 cm); segment 2 (3.0 x 2.4 cm) and segment 5/6 (2.5 x 4.3 cm). No suspicious hypermetabolic pulmonay nodules are detected. Multiple FDG avid lymph nodes in the abdomen – peri-portal regions (size of 2.2 x 2.8 cm); retrocaval (1.8cm) and aorto-caval regioin (1.8 cm).
The doctor asked my father to undergo chemotherapy again or take oral chemo drug. My father refused to do both.
Total Cost of Treatment
The chemo treatment came to about 1.5 billion rupiah (approximately RM 0.5 million). The surgery cost an additional 0.4 plus billion rupiah. So the total cost of 2 years of treatment in Singapore came to about 2 billion rupiah.
Comments
Is this story unique? Not at all. It happened most of the time with lung cancer patients. Story 5 in our book, Lung Cancer – What Now? tells of a lung cancer patient who underwent similar treatment by the same doctor! The family spent 8 billion rupiah (approximately SGD 1 million). The result: The same, disastrous ending. He died soon after coming to see us.
Over the years dealing with patients, I began to see a very clear pattern emerging in the medical treatment for lung cancer. If you wish to know more, just read the following and learn to become an empowered patient. Perhaps you don’t have to die suffering and at the same time leave a “big hole” in your bank account.

Available: http://bookoncancer.com/productDetail.php?P_Id=75

(Available http://bookoncancer.com/productDetail.php?P_Id=73)
Review by Yeong Sek Yee & Khadijah Shaari

Jacqueline Kennedy Onassis, just like the late Senator Hubert Humphrey, also died a painful death in May 1994. Jacqueline Kennedy was the wife of the late President John Kennedy, the 35th President of the USA from January 1961 until he was assassinated in November 1963. Jacqueline subsequently married Greek shipping tycoon Aristotle Onassis in 1968 and was later known as Jacqueline Kennedy Onassis.
Mrs. Onassis was healthy until early December1993, when she noticed a swelling in her right groin. A doctor diagnosed a swollen lymph node, and suspecting an infection, prescribed antibiotics. The swelling diminished but did not completely disappear. While on a boat cruise in the Caribbean over the Christmas holidays in 1993, Mrs. Onassis developed a cough and swollen lymph nodes in her neck and pain in her abdomen.
Subsequently another doctor found enlarged lymph nodes in her neck and in her armpit. A CAT scan, showed that there were swollen lymph nodes in her chest and in an area deep in the abdomen, the retroperitoneal area.A biopsy of one of the neck nodes showed that Mrs. Onassis had non-Hodgkin’s lymphoma (NHL).
In early January1994, Mrs. Onassis began receiving the first of four standard courses of chemotherapy for the lymphoma. The therapy included steroid drugs, and the initial treatment led to an apparent remission. But in mid-March 1994, she developed weakness, became confused and had pains in her legs. A neurological examination indicated that the cerebellum portion of her brain had been affected. Later, an M.R.I. showed that the lymphoma had disappeared from her neck, chest and abdomen but that it had spread to the membranes that cover the brain and spinal cord.
After the cancer was found in her brain, Mrs. Onassis received radiation therapy there and to her lower spinal cord for about a month. The treatment relieved her weakness, but she continued to experience pain in her neck, for which she was given pain medications. During this time she received her care at home and as a hospital out-patient.
On April 14, Mrs. Onassis was admitted to New York Hospital-Cornell Medical Center after she developed a perforated ulcer in her stomach, a complication of the steroid therapy. Surgeons sewed up the hole in the stomach that day.
However the cancer in her spinal cord and brain continued to worsen. Although a tube was placed in her brain to deliver an anti-cancer drug, a sophisticated but now standard form of therapy for this condition, the lymphoma in her brain did not respond to any therapy. During this period, she lost weight, her speech slowed; she was less alert and had difficulty walking.
A subsequent CAT scan showed that the lymphoma was in her liver in huge amounts.Doctors said there was nothing else medicine could offer. After consultation with her family and in keeping with the intent of her living will, Mrs. Onassis asked to go home from the hospital.
The above was reported in the New York Times of May 20 1994 (read article at following link http://www.nytimes.com/1994/05/20/us/death-of-a-first-lady-no-more-could-be-done-mrs-onassis-was-told.html).
Harvey Diamond, in his best seller FIT FOR LIFE, A NEW BEGINNING, was more explicit in his description of Mrs. Onassis’s battle with lymphoma…the following are excerpts from the book:
…..she was bombarded with drugs. Lots of powerful, virulent, energy-sapping, life-diminishing drugs. The New York Times stated that she “initially responded to therapy, but it (cancer) came back in her brain and spread through her body”
For the unrelenting pain in her neck, Mrs. Onassis received more drugs. For the acute pneumonia she developed in her weakened state, she received more drugs. Steroids were part of the mixture in her chemotherapy, which caused a perforated ulcer in her stomach. In the middle of her ordeal, she had to be operated on to sew up the hole in her stomach. She went from bad to worse, and as a final assault on her body, she was subjected to even more radiation and chemotherapy, only this time it was shot directly into her brain. The cancer spread to her spinal cord, her liver, and throughout her body. She became weak and disoriented, lost weight, developed shaking chills, her speech slowed, and she had difficulty walking.
A POINT TO PONDER
Mrs. Onassis was diagnosed with NHL in January 1994 and she passed away on May 19 1994…just barely 5 months after diagnosis/treatments. Why did she have to die such a painful death? Did the scientifically tested, proven and evidence-based cancer treatments caused the cancer to spread? Or was the NHL too aggressive?
We leave it to you to be the judge.
DK (S-542) is a 63-year old lady from Sumatera Selatan. She found a lump in her right breast. She ignored it for about 3 to 4 years since it did not give her any problem. In July 2008, she started to have pain and the lump grew bigger.
Two years later, in November 2010, DK went to a hospital in Melaka (Malaysia). She was asked to undergo an operation. She was afraid and went home instead. Then she sought alternative treatment. She went to Central Java and sought the help of a herbalist who gave her herbs to apply and also “massaged” her. The treatment expelled pus and blood from her breast. For the first 6 months, the treatment seemed to help DK.
Since she felt well, DK went to China for a holiday. While in China, she suffered severe pain and her condition deteriorated. On her return to Indonesia she was admitted to a hospital in Jambi. CT and biopsy were performed. DK subsequently underwent 7 cycles of chemotherapy, followed by a mastectomy. After surgery, DK was put on Tamoxifen and Xeloda. She was on these two drugs for about 7 to 8 months. After 2 months on the drug, her right arm became swollen and a big blister developed (Picture A). She had difficulty bending her fingers (Picture B).

DK stopped taking Tamoxifen and Xeloda. She went back to see her doctor again in February 2014. The doctor prescribed painkiller. By this time there was also a swelling in her neck (Picture C). The doctor told her there was nothing he could do to help her. Desperate, DK’s son found us in the internet. On 7 March 2014, DK, her husband and son came to seek our help.
DK was prescribed Capsule A, C and D. In addition she was asked to drink herbal teas: Breast M, Lympho 1, Upper Edema and Pain Tea.
One Month On The Herbs
DK’s son came to report his mother’s progress on 9 April 2014.
1. DK did not seem to have any reaction after taking the herbs for the first 3 days.
2. On day 4 after taking the herbs, DK had severe pain in her right arm. The pain lasted untill 1 or 2 a.m. Her right leg felt sore and numb.
3. She passed out black stools with a lot of mucus. After that she passed out stools with oily discharge.
4. One week on the herbs, the pains in her right arm became less, soreness in her right leg also lessened.
5. Before the herbs, DK was on morphine, 2 tablets per day. After a week on the herbs, she did not need morphine anymore.
6. Two weeks on the Upper Edema tea, the swelling of her right arm improved. It became smaller and soft (previously hard). But after stopping the Upper Edema tea, the swelling came back.
7. DK was able to sleep well throughout the night. Previously she could sleep for only about 2 hours each night.
8. Her appetite had improved and she could eat rice.
9. She had more energy.
Comments: There are many lessons we can learn from DK’s bitter experience.
1. Ladies, if you have a lump in your breast. it is prudent for you to go and get an ultrasound done and determine if the lump is benign or malignant. If it is malignant, it makes no sense to keep it in your breast. Don’t be fooled by those who want you to believe that their “treatment” can cure you. I have heard of the Kiss Therapy, Leech Therapy, etc. which did not work. There is no reason for you to delay removal of the cancerous breast. The longer you wait the more problems you are going to create for yourself later on. Like in DK’s case, she delayed and delayed but ended up having to remove her breast anyway. By that time it was too late.
2. If you go and see your doctors with a large lump in your breast, the first thing they would want to do is chemo you! DK had to endure 7 cycles of chemo before a mastectomy was performed. If she was to go and see the doctor earlier she would not need to do the chemo at all – proceed straight to lumpectomy or mastectomy.
3. After the mastectomy, DK was put on Tamoxifen and Xeloda and she was on these drugs for about 7 to 8 months. This is something that blew my mind off. Why Xeloda? Why Tamoxifen? Can someone not learn from simple observation? Learn from DK’s experience (and many others like her) that these drugs have never been shown to cure cancer! In DK’s case, things got worse, not better.
4. When DK went back to her doctor for more help, she was only given Morphine tablets, nothing else. The doctor told her son, “There is nothing else I can do to help your mother!” At least the doctor was being honest. Perhaps other doctors would suggest, “Do more chemo!” But the question to ask is: Can more chemo cure this metastatic cancer? Before Amy Cohen Soscia died, she left this remark for the world to learn, “There is no cure for metastatic breast cancer. It never goes away. You just move from treatment to treatment.”
5. As usually, at this “terminal stage” when there is nowhere else to go, patients come to seek our help. In spite of this dire situation, some expect us to cure them — see how absurd or illogical it is! But some patients come hoping that we can help them attain a better quality life with no pain. Yes, this is more realistic and as in DK’s case (and numerous other cases like hers) we are able to help. So even if your doctors give up on you (like DK), know that there is still another option for you to get well. So don’t give up. That is, if you are prepared to help yourself.
6. Unfortunately, not all patients who come to us want to help themselves. They expect healing to come easy! Or they want healing on their own terms. Many just want to sit in the comfort of their home and expect us to “deliver healing via e-mail.”
Let me point out to you what DK and her family had to go through to come to us. They live in a town that takes 7 hours to drive to Jambi. From Jambi they have to take a plane to Jakarta and from Jakarta they have to fly to Penang. In all, the one way journey from home to Penang takes 2 days!
We often have requests to have phone consultation because patients live “far away and cannot come.” When we ask from where? Ah, the answer is BM, Taiping or Ipoh (just one or two hours ride across the Penang bridge) or even Singapore (one hour and a half by plane). For those who what to find easy healing, our advice is to find someone near your home to help you. It is more convenient for you.
7. Following our healing path is not like going for a honeymoon trip. First, you must take full responsibility for your health. Change your lifestyle. Change your diet. You need to brew the teas and drink the bitter concoctions ( Some people ask, why not have them in capsules?). Probably for a week or two after taking the herbs, you have to go through a “healing crisis.” You may have more pain, more discomforts, etc. After this healing crisis you will probably feel better, as in the case of DK and many others like her. To learn more about healing crisis, click this link: http://www.cacare.com/healing-crisis
8. Most patients who come to us often claim that they are ignorant — “I don’t know.” “We panic, we are confused and don’t know what to do.” “They never tell me all these things.”
In order to educate patients, I have written another book on breast cancer (below):

(Available at http://www.BookOnCancer.com)
This book provides you with all the essential information that you need to know and tell you exactly what to do if you have a lump in your breast, etc. etc. Pleading ignorance is no excuse. You have a choice. And your life is in your hands. Do what is right.
LKF (E324) is a 32-year-old male. Sometime in June 2013, he passed out blood in his urine. USG of the abdomen showed a large right renal mass suspicious of renal cell carcinoma. He was asked to go for CT scan but decline due to financial constraint. In early 2014, he started to cough, sometimes with blood stain sputum. He had shortness of breath, chest pain and hoarse voice. LKF was referred to the respiratory unit of the general hospital. CT showed metastatic lung cancer, the primary was probably from the kidney. Because of right pleural effusion, pleural tapping was done. Bronchoscopy and biopsy were performed and confirmed cancer. LKF was subsequently referred to the oncology and urology units for further management. He was told that he might have to undergo chemotherapy (expensive drug which he could not afford) and later an operation to remove his cancerous, right kidney. 
I explained to LKF and his sisters that this is a Stage 4 cancer and I would try to best to help, but don’t expect magic from us. LKF was prescribed herbs: Capsule A, C and D and herbal teas: Kidney, Lung 1 & 2, Lung Phlegm, deTOX + WF.
ONE WEEK ON HERBS
After one week on the herbs, LKF and his sisters came back to see us again and reported a real unique and strange response to the herbs. 1. After 3 days on the herbs, LKF passed out a worm or parasite when he urinated. It was about 8 inches long and the thickness about the size of the index finger. At first only the “head” protruded out and he had to pull it out through the urethra. It was rubbery. Unfortunately, he threw away the specimen. I reminded him if this happened again, he should keep the specimen and let me have a look at it. 2. LKF also passed out blood clots once a while when urinating. The blood clot discharged was jelly-like and came out in big pieces. This actually blocked his urine flow. When he felt his bladder was truly full he tried to push out his urine and with that the clot was also pushed out. This is the jelly-like blood clot he expelled while urinating. 
TWO WEEKS ON HERBS
LKF and his sisters came to see us again on 4 April 2014. 1. He have been coughing for about 3 days. Suddenly he coughed out a “worm.” This time it was from the lung not from the urinary bladder. 2. After he expelled this worm, he felt better – more alert and had more energy. 3. During these two weeks, he did not expel any more worm while urinating but he did pass out blood clots once a while when he urinated. This time, LKF brought along the specimens for us to see.  The “worm” expelled after coughing (above) is much smaller than the one he expelled while urinating last week.
The “worm” expelled after coughing (above) is much smaller than the one he expelled while urinating last week.
Comments:
This is indeed a strange incident. Although I have read that parasites could cause cancer, I have never come across such case before. That led me to browse through the internet for more information. And let me share with you what I learned.
1. It is true that we harbour parasites in us. Time to deworm ourself once a while?
2. Trematodes are known to be able to cause cancer. Example of liver flukes, Opisthorchis are said to dramatically increase risk of liver cancer, schistosoma dramatically increase risk of bladder cancer and male breast cancer.
3. About 200 million people across 75 of the poorest countries in the world are now infected by the blood parasite Schistosoma haematobium (S. haematobium). The worms enter the blood stream and release eggs that become embedded in the bladder wall where they cause chronic inflammation and, in some patients, lead to bladder cancer. The adult worm can also migrate to its preferred body part, depending on its species. These areas include the bladder, rectum, intestines, liver, portal venous system (the veins that carry blood from the intestines to liver), spleen, and lungs. It is common in many tropical and subtropical areas worldwide.
4. These parasites can cause various complications such as: Bladder cancer, Chronic kidney failure, Chronic liver damage and an enlarged spleen, colon (large intestine) inflammation with bloody diarrhea, Kidney and bladder obstruction, Pulmonary hypertension, and Right-sided heart failure.

You must be logged in to post a comment.