
KDL is a 55-year-old Indonesian lady. For the past 10 years she had been having problems of “wind” in her abdomen. She consulted doctors for this problem and was prescribed medications. Unfortunately these did not solve her problems.
Eventually in June 2014, KDL went to a hospital in Johor. The doctor did a scope and found nothing! She was again prescribed medications but they were not effective.
In November 2014, KDL went to a private hospital in Melaka. A CT scan was done. The findings were:
- Multiple liver nodules in both lobes, predominantly right lobe. The largest is 3.3 x 3.4 cm in segment 8.
- Extensive intra-abdominal adenopathies involving porta, coeliac and para-aortic nodes — largest being 1.2 x 1.6 cm, in retropancreatic region.
- Normal gallbladder configuration is not demonstrated. Hetergenous wall thickening seen.
Conclusion: CT features of gallbladder raises the possibility of GB malignancy with metastatic liver nodules and intra-abdominal adenopathies.
No surgery was indicated. KDL was prescribed an oral chemo-drug, Xeloda. This cost her RM 2,400 per cycle. A cycle consisted of taking 5 tablets per day for 2 weeks followed by a week of rest.
One year later, 27 July 2015, a CT scan was done and the result showed:
- Several heterogenous hypodense nodules in bilateral lobes — largest is 4 x 4 x 3.5 cm in segment 8. (note: this has grown bigger).
An X-ray of the chest showed:
- Several ill defined lung opacities of sizes from a few mm to 15 mm.
- A 2 cm right hilar opacity also seen.
Impression: Suspicious of lung and right hilar secondaries.
Blood test showed:
| CEA | 135.0 (High) |
| CA 125 | 388.0 (High) |
| CA 19.9 | 179.0 (High) |
KDL said that after a year of taking Xeloda her condition became worse!
- She developed sleeping difficulties.
- Her stomach was very uncomfortable, with “wind” moving around.
- Her backbone felt numb / sore.
Comments
This is indeed a very sad story — and is this also a story of bad management?
Why bad management?
- KDL has been having “wind” problems for the past 10 years. Why was her problem not correctly diagnosed in spite of her consulting the doctors even at an early stage?
- One lesson we can learn from this case is, If you go to your doctor and was told that there is nothing wrong — please know that you may be in trouble later! That is, if after taking the doctor’s medication the problem still persisted. Again, don’t take “NO problem” as a good answer. Go and find 2 or 3 more doctors who may be able to do a better job.
- Her stomach “wind” problems could be an early sign that something serious was coming. Could it be problems related to the pancreas? stomach or colon? or ovary? But, at the early stage, no one bothered to properly diagnose her — only prescribing drugs after drugs which did not work.
- KDL’s problem was left to simmer for too long. Then 10 years later, someone decided to do a CT scan. Why wait for 10 years to do a scan? By that time it was too late, it was already a disaster.

After the CT scan the doctor could not do much, except to offer KDL Xeloda, which she faithfully took for a year. Xeloda made her worse off — physically and financially!
The question we may want to pose is: What can Xeloda do for KDL? Realistically, what do you expect to achieve from consuming Xeloda? Would Xeloda do more harm than good?
Would it not be better if the doctor just send KDL home without any medication? To most people — patients, their family members and doctors — this suggestion may sound ridiculous, “madness” and unacceptable. But hang on, read this article and see if you can learn anything from it.

For 25 years, the professor was studying the effects of chemotherapy and came to a horrifying conclusion!
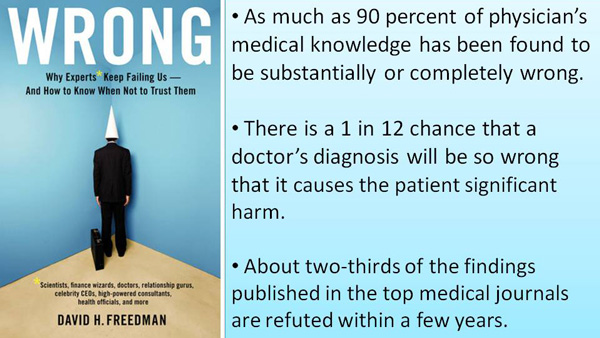
The cancer industry is just an industry after all! Doctors, hospitals, pharmaceutical companies and other stakeholders in this industry profit whenever a patient accepts the toxic treatment that is chemotherapy, radiation or surgery …. despite the claims from the medical industry that chemotherapy does not work in the fight against cancer.
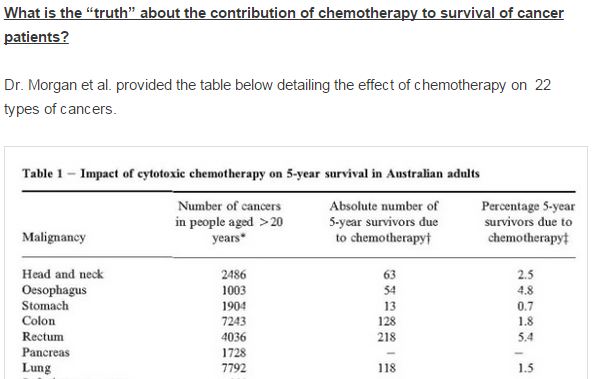
Dr. Hardin B. Jones, a former professor of medical physics and physiology at the University of California, Berkeley, has studied the life expectancy of cancer patients for more than 25 years, when he concluded that chemotherapy does not work.
He testified that chemotherapy patients often die a horrible death. They also died much faster and more painful than patients who opted for a different approach. What he found was that chemotherapy actually shortened the life and killed patients, and everything is kept secret because of the millions of dollars in play!
“People who refused chemotherapy treatment live an average of 12 and a half years longer than the people who are receiving chemotherapy,” Dr. Johns said in his study published in the New York Academy of Sciences. “People who accept chemotherapy die within 3 years, and many just a few weeks after starting the treatment.” “Patients with breast cancer who reject conventional therapy live four times longer than those who follow the system. This is something you will not hear in the mass media that will continue to spread the myth that chemotherapy is the best medicine to fight cancer!”
Modern medicine hides the truth about cancer therapy. One treatment costs 300000-1000000$! That is why it continues offering chemotherapy to cancer patients. Chemotherapy does not remove cancer nor extend the life. It just burdens the body so much that the patients eventually die from it.
After putting full faith in the doctors, KDL and her family finally realised that it was a big mistake. KDL stopped taking Xeloda. KDL’s son started to surf the net and found CA Care. Then the family came to Penang in late October 2015 to seek our help.
When KDL came into our centre, I asked if she had a “stroke” before. She said, No. But since the past 2 weeks, she was not able to lift up her left arm. She walked dragging her left leg. Her walk was unstable. One question came to mind, Has her cancer gone to her brain? An X-ray on 27 July 2015, showed lung metastasis. Or, could Xeloda have caused a blood clot leading to a stroke — could this be the reason why she presented as such?
We discussed the possibility of a brain metastasis. To know for sure, a CT or MRI of the brain may be indicated. But, what is the use of spending more money just to know if there is something in the brain? Okay, after the scan, can anyone cure her? There are enough tumours in KDL’s liver and lungs to worry about anyway.
Since herbs are not poisonous like chemo-drugs, KDL was given teas for her liver, lungs and brain. We told her: Let’s see what happen after a month.
Lack of Knowledge
When KDL and her family came to see us, we understood why she was “neglected” and left in such a limbo. She and her family were not educated. They trusted their doctors and have full faith in them. They did not know how to ask questions. They were clueless about their problem. They believed KDL was given the “best” treatment.
Indeed we felt very sorry for KDL and her family.
Let us repeat what we have always said to patients. Please read and learn. If you choose to know nothing about your health and put your full belief and trust that others can help you, know that you may end up “a dead duck.” So, patients, please empower yourself. But in KDL’s case, we understood. She was not educated. She was helpless and naive. She needed help.
Another case: Xeloda did not stop recurrence of colon cancer
As we were dealing with KDL case, a friend dropped by our centre. He is 70 years old and was diagnosed with rectosigmoid cancer in October 2014. He underwent a surgery and the histopathology report indicated a Duke Stage B cancer with no spread to the nodes or other parts of the body. The patient was given Xeloda which he took faithfully.
Barely a year later, October 2015, the cancer recurred. The patient underwent another surgery. The histopathology report confirmed a moderately differentiated adenocarcinoma of the colon, recurrent in the abdominal wall.
This patient took Xeloda, but was Xeloda useful for him? It did not stop the cancer from coming back. Our friend decided not to undergo further chemotherapy and came to us for help.
What is Xeloda?

This is the “in thing” drug of today, being prescribed to patients with various cancers. Let me give you what they say about Xeloda in the net.
Xeloda is its brand name. Its generic name is Capecitabine. It is used to treat advanced metastatic breast cancer, colon cancer, and many other cancers.
Xeloda is taken as a pill and when inside the body is converted to 5-FU (5-fluorouracil). Since 1957 – 1980s researchers and doctors were experimenting and treating cancer with 5-FU. Therefore 5-FU is actually an old drug, used to treat colon and rectal cancer, breast cancer, anal, esophageal, pancreas and gastric (stomach) cancer, head and neck cancer, liver cancer, ovarian cancer, etc. This is given as injection, not taken orally like Xeloda.
So it reality, 5-FU is an old drug. But Xeloda is considered a “newer drug” although it is the same old thing. So can we say that Xeloda is like an old wine packed in a new bottle?
Another drug which is like Xeloda is UFT (tegafur plus uracil). UFT is not popularly prescribed yet but perhaps one day someone may decide to make it as popular as Xeloda and push it for cancer treatment.
Why is Xeloda popularly prescribed?
I think it is because it is easy to use. Just send patients home and ask them to swallow the pill and you get 5-FU inside the body. Before Xeloda, drug like 5-FU, had to be given as an injection. So there is a lot of hassle. Also, chemo-injection has already earned a “notorious” reputation of causing adverse side effects. So, giving patients a new “form” of the same drug perhaps would be a better strategy. Most patients may not even know that Xeloda is a chemo-drug anyway! So, the treatment would not sound as scary as the dreaded “chemotherapy.”
The one most important question to ask is, Can 5-FU or Xeloda cure cancer?
Well, if it is effective people would not die of cancer then.
We got to know 5-FU since the 1990s. Two of our patients who had colon cancer were treated with 5-FU. They died. Even today, as you can see from the above stories, patients who took Xeloda did not get any cure.
Side effects of Xeloda`
- Fatigue
- Diarrhea
- Hand -foot syndrome -skin rash, swelling, redness, pain and/or peeling of the skin on the palms of hands and soles of feet. Usually mild, start as early as 2 weeks after start of treatment.
- Nausea and vomiting
- Dermatitis
- Elevated liver enzymes (increased bilirubin levels)
- Poor appetite
- Abdominal pain
- Low white blood cell count.
- Low red blood cell count (anemia)
- Low platelet count.
- Mouth sores
- Numbness or tingling of hands or feet
- Swelling of the feet and ankles
- Fever
- Constipation
- Eye irritation (watery eyes, inflammation of the eyelids, redness).
- Shortness of breath
- Headache
- Chest, back, muscle, joint, bone pain
- Dizziness
- Insomnia (sleep disturbances)
- Excessive sleepiness, confusion, very rare seizures
- Dehydration
- Cough
- Blood clots (Blood clots rarely can lead to pulmonary embolus or stroke)
- Loss of balance
- Nail changes, darkening of the skin
- Taste changes
(Reflect on what happened to KDL after taking Xeloda for a year. Take note of the side effects written in red)
Yes, doctors who prescribe Xeloda would say this drug will do you a lot of good. So, go ahead and believe them and hope for the best!
Here are other views on Xeloda that I got from the internet.
Xeloda killed my mother: http://www.rxlist.com/script/main/rxlist_view_comments.asp?drug=xeloda&questionid=fdb7906_pem
- Xeloda killed my mother. She died on December 27th, 2007, ten weeks after starting a Xeloda regimen. She was 83, and she was in very good shape before beginning her treatment, in spite of the presence of secondary liver cancer (breast cancer metastasis). The drug destroyed the lining of her digestive system, and allowed a combination of bacterial infections to attack and kill a portion of her small intestine. She was within hours of death when emergency surgery repaired her intestine on 11/24/07. It appeared as though she would recover from her surgery, but she contracted pneumonia while hospitalized, and her system was too weak to fight back. I am heartbroken. I don’t want my mother’s death to prevent others from seeking proper treatment, but everyone should be aware of the dangers presented by bacterial infections that could cause major damage while this drug is being administered. James W. Moore jim@ed2c.com
Side effects of Xeloda
- I have been taking Xeloda for over 6 months. My side effects began with very much pain in every part of my body … I have developed hand-foot syndrome. I’ve lost all the skin of the bottoms of my feet and I’m now my hands are peeling. My feet and hands are very sensitive to anything with a texture. I even have trouble opening a water bottle. Sometimes I want to stick my feet in buckets of ice! …. I just recently developed severe eye irritation which I brushed off as bad contacts or pollen in my eyes. I finally went to my eye doctor and he found severe eye irritation and swelling in my cornea. After speaking with a corneal specialist, he determined it was the result of taking Xeloda.
- I have been on Xeloda for 3 years. I have the cancer cells in my left lung and spine, hip and left leg bones. Stage 4. Some new growth in the bones but no new growth in the left lung and no fluid build-up. I also have the hand and foot symptoms and sometimes I cannot walk and my hands are so smooth and sore I can’t even hold an envelope. Wear gloves most of the time and us a cane. BUT, life does not stop and neither should you. I still travel air, sea and land. And I have lots of praying friends and family. I have also changed my diet. NO SUGAR and very little meat mostly vegetables and fruit, organic if I can. Go till the Lord calls you home.
- Xeloda is sort of an odd drug. For most people, it is viewed as an “easy” drug which is quite effective. For others, including me, it is more problematic. Usually, side effects start appearing in 7 – 10 days. For me, they start getting bad on about day 10 and it lasts through day 21, getting slightly better, but never going completely away, depending on the particular side effect.
- The most common side effect is … hand and foot syndrome … Hand and foot syndrome with Xeloda is the redness and tenderness of the hands and feet. With me, I slough off skin, bit sheets of skin on my hands and feet. They become tender, and have a burning sensation. In addition, they swell and feel tight. It is not unusual for the heels, toes and sides of the feet to develop deep fissures or cracks. Up to 60% of the patients taking Xeloda suffer from this, and it varies in severity.
- When I first started taking the correct dosage of 4,000 mg a day … two weeks on and one week off, I had massive issues. I had diarrhea, gas, nausea, and constipation (yes, even while I had the diarrhea), dehydration, dry eyes, dry mouth (cotton mouth), cramping, stomach pain, loss of appetite. It was severe enough that the oncologist backed it off to 3,000 mg. a day That took care of the most severe problems–the nausea, and diarrhea and stomach pain.
- With 3,000 mg. a day, I still have: periodic constipation, hand and foot syndrome, vision changes (dry eyes which makes things sort of hard to focus on), dry mouth/cotton mouth, lack of taste, toxicity rash (the rash you see in the bottom picture which can also blister and tear easily…I call them my toxicity evening gloves), thinning hair (boy is this one annoying! I just got hair back and then I started to lose it again!), sensitivity to the sun, higher blood pressure than I usually do, discoloration of my nails and the worsening of a nail fungus, fatigue, anemia, heart burn. My feet also often get little blood blisters, which my onc says is probably because my skin is so thin…you bump it, and then you get a blister. Fortunately, I only had mouth sores (stomatitis) once.
- I had breast cancer in 2000 which had spread to my spine in one of my vertebrae. I was prescribed Xeloda by my oncologist. Despite the severe side effects of hands and feet going red, blisters in my mouth and skin disorders, the oncologist insisted on this drug. I decided to terminate the use within 11 weeks. I am now experiencing numbness in both my hands, swelling and stiffness in all the joints of my hands. I believe patients should be warned about these side effects so that they understand the risks involved in taking such severe treatments. These side effects may take six months or even a year to appear.
Source: http://www.webmd.com/drugs/drugreview-7906-Xeloda+Oral.aspx?drugid=7906&drugname=Xeloda+Oral
To round up, here are the links to stories of some patients who came to us after taking Xeloda.
2. Breast Cancer: Surgery, Chemo, Tamoxifen and Xeloda failed her!
- Leo was not convinced that Xeloda would do him any good. He had fevers and diarrhea. In addition he vomited and had pains around the colostomy stoma after taking Xeloda. https://cancercaremalaysia.com/2013/12/25/dissecting-chemotherapy-15-couldnt-afford-avastin-gave-up-xeloda/












































You must be logged in to post a comment.