
Jack (not real name) was 43 years old when he was diagnosed with lung cancer. His problem started in October 2013, when there was a swelling in the right collar bone. Apart from this, there was no other symptoms — no cough, etc. Jack said in 2013, he had fevers on three occasions that make him feel tired.
A blood test on 24 October 2013 showed his CEA was at 133.3 and CA 19.9 at 9,524.0
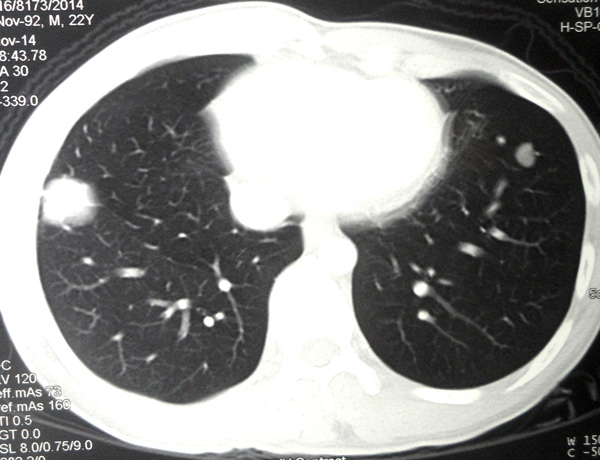
A CT scan on 30 October 2013 showed:
- An irregular lesion in the right lung apex, 35 x 42 x 28 mm.
- Speckles of calcification in both lungs upper lobe suggesting prior tuberculous infection.
- Bilateral supraclavicular lymph node 10 to 20 mm.
- Multiple enlarged mediastinal and right hilar lymph nodes.
- Numerous small nodules in both lungs – likely metastases.
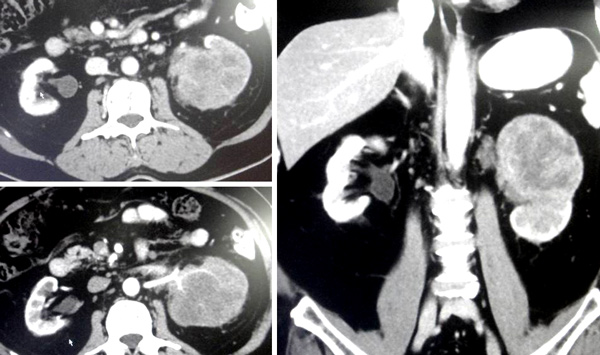
- Liver shows a least 7 hypodense lesions, largest 30 x 32 mm in the left lobe – likely metastases.
- Multiple enlarged lymph nodes in the celiac and paracaval regions.
- Sclerotic lesions at vertebral bodies of L3, L4 and L5 – likely metastases.
A tru-cut biopsy of the right lung mass was performed and confirmed a moderately differentiated adenocarcinoma.
Jack underwent 6 cycles of chemotherapy. The drug used was Cisplatin. Each cycles cost about RM10,000. The treatment lasted until February 2014.
Let’s follow the progress of Jack’s treatment.
Table 1: Blood test results during chemotherapy.
| Date | 24 Oct 13 | 25 Nov 13 | 16 Dec 13 | 6 Jan 14 | 27 Jan 14 | 17 Feb 14 |
| Total bilirubin | 18.1 H | 13.7 | 15.5 | 13.5 | 14.8 | 17.8 |
| Alkaline phosphatase | 210 H | 217 | 147 | 132 (normal) | 148 | 125 |
| ALT | 49 | 62 | 59 | 34 | 26 | 23 |
| AST | 28 | 30 | 30 | 21 | 19 | 17 |
| GGT | 114 H | n/a | n/a | n/a | n/a | n/a |
| Platelet | 495 H | 477 | 250 | 258 | 233 | |
| CEA | 133.3 H | n/a | n/a | n/a | n/a | n/a |
| CA 19.9 | 9,524 H | 2,394 | 325 | 268 | 246 | 195 |
| Before chemo | After chemotherapy | |||||
| At this stage, chemotherapy was very effective and helpful. Alkaline phosphatase declined. Platelet count was down and CA 19.9 decreased from 9,524 to 195. Bravo – great results. | ||||||
After the completion of chemotherapy in February 2014, Jack was put on the oral drug Tarceva. He was on Tarceva until June 2015.
His tumour markers – both the CEA and CA 19.9, continued to decrease (Table 2).
Table 2: After intravenous chemo, patient was on oral drug, Tarceva.
| Date | 25 Mar 14 | 15 Apr 14 | 14 May 14 | 16 Jun 14 | 21 July 14 | 18 Aug 14 |
| Total bilirubin | 31.6 | 37.7 | 27.5 | 25.5 | 24.6 | 27.8 |
| Alakaline phosphatase | 142 | 136 | 125 | 84 | 78 | 66 |
| ALT | 26 | 43 | 36 | 17 | 16 | 14 |
| AST | 27 | 56 | 24 | 20 | 19 | 16 |
| GGT | n/a | n/a | 40 | 26 | 23 | 23 |
| Platelet | 370 | 253 | 281 | 313 | 266 | 281 |
| CEA | n/a | 28 | 2.3 | 1.9 | 1.6 | 1.4 |
| CA 19.9 | n/a | 14 | 5.0 | 6.5 | <2.0 | 3.8 |
| Six months on Tarceva (from February 2014 to August 2014) the CEA and CA 19.9 decreased significantly.Again, great results! | ||||||
From April 2014 to December 2014 Jack also received 6 to 8 monthly injections of Denosumab. This is a monoclonal antibody used to treat bone cancer. It is also known by its brand name, Xgeva and Prolia.
Table 3: CEA and CA 19.9 started to increase even though Jack was on Tarceva.
| Date | 22 Sep 14 | 20 Oct 14 | 24 Nov 14 | 29 Dec 14 |
| Total bilirubin | 21.8 | 21.6 | 21.9 | 27.1 |
| Alakaline phosphatase | 66 | 76 | 69 | 77 |
| ALT | 16 | 15 | 16 | 16 |
| AST | 18 | 22 | 19 | 20 |
| GGT | 23 | 23 | 26 | 24 |
| Platelet | 277 | 329 | 294 | 299 |
| CEA | 2.2 | 3.9 | 7.4 | 12.6 |
| CA 19.9 | 7.2 | 6.6 | 11.4 | 27.9 |
| From September 2014 both the CEA and CA 19.9 started to increase in spite of Jack being on Tarceva. In September 2014 the CEA was 2.2 and it increased to 12.6 by December 2014. Similarly, CA 19.9 increased from 7.2 to 27.9 during the same period. | ||||
Because of the rising CEA and CA 19.9, Jack was again given 4 cycles of chemo. This time the drugs used were Carboplatin + Gemzar. The total treatment cost RM40,000.
Table 4: The second round of chemo with Carboplatin + Gemzar produced limited benefits.
| Date | 26 Jan 15 | 27 Feb 15 | 6 Mar 15 | 13 Mar 15 | 27 Mar 15 |
| Total bilirubin | 24.6 | 17.6 | 19.9 | 15.6 | 24.7 |
| Alakaline phosphatase | 74 | 87 | 54 | 67 | 61 |
| ALT | 16 | 19 | 25 | 20 | 15 |
| AST | 21 | 17 | 16 | 16 | 14 |
| GGT | 27 | 27 | 27 | 27 | 23 |
| Platelet | 315 | 295 | 453 | 192 | 259 |
| CEA | 22.3 | 21.6 | 22.0 | 28.6 | 29.9 |
| CA 19.9 | 47.2 | 44.6 | 31.9 | 52.5 | 70.2 |
| From January to April 2015, Carboplatin + Gemzar regime managed to stabalized the CEA level ranging from 22 to 30. CA19.9 stabalized from 31 to 70 during the same period. | |||||
Table 5: CEA and CA19.9 on the march — treatment failed!
| Date | 3 Apr 15 | 17 Apr 15 | 24 Apr 15 | 19 Jun 15 |
| Total bilirubin | 20.4 | 25.8 | 24.8 | 33.7 |
| Alakaline phosphatase | 49 | 73 | 65 | 73 |
| ALT | 24 | 14 | 23 | 12 |
| AST | 16 | 14 | 18 | 14 |
| GGT | 24 | 22 | 24 | 24 |
| Platelet | 509 | 276 | 268 | 321 |
| CEA | 29.6 | 32.7 | 31.6 | 93.2 |
| CA 19.9 | 45.1 | 52.5 | 37.7 | 511.5 |
| Error in platelet reading? | In April CEA was around 29 to 31 while CA 19.9 was around 37 to 45.But barely 2 months after the completion of chemotherapy, the CEA shot up to 93.2 and CA19.9 went up to 511. | |||
Jack said he was disappointed with the results, in spite of the initial good response to chemotherapy. He decided to “shop” for alternative medicine while waiting for his doctor to take the next step.
Comments
This is indeed a sad case but not a unique one. Over the years we have seen cases after cases like this. After the chemo, the tumour markers dropped or the tumour shrunk or disappeared. But such responses did not last long. After a few months, the cancer recurred and this time it became more aggressive.
We sat down with Jack and tried to understand what was going on. No doubt about it, he was very much encouraged with the initial results. Within 8 months of treatment his CA 19.9 which was at 9,524 dropped to less than 2.0. That was a great achievement indeed. Who would not be excited about such feat? But what many patients don’t know or what those who should know do not want to know is that such dramatic drop of CA 19.9 (or even total shrinkage of tumour) is not permanent. It NEVER translates into a cure. It is meaningful in the short term but meaningless in the long term.
Read some of the stories here:
https://cancercaremalaysia.com/2014/07/05/the-story-of-moms-lung-brain-bone-cancer/
https://cancercaremalaysia.com/2013/11/29/lung-cancer-chemo-experiments-that-failed-and-failed/
Let me ask you to ponder what Einstein wrote:

Do you see any truth is that statement?
Many of us may want to ask: Where is the problem? What causes this problem? What can we do about it?
Jack told us that his oncologist is a very nice man and he was trying his best to cure him. Understandable. We cannot blame the doctor. Legally and medically, apart from chemo or oral drugs, he has nothing else to offer you. He can’t ask you to take supplements or herbs, etc.
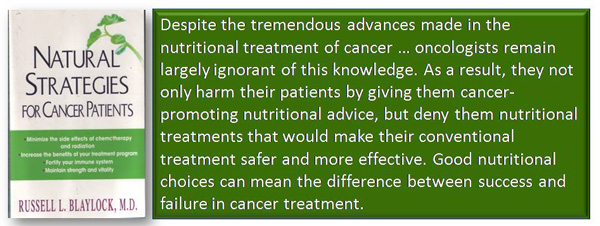
Unfortunately, some oncologists will rip apart those who dare to suggest that patients take herbs, vitamins or control their diet. Nonsense they say — all these non-medical ways are not scientifically proven.
But hang on, is the present day treatment like above based on “real science”? Granted, these chemo-drugs have undergone clinical trials and have been approved by Government Authorities. But, what does all this mean? The approved drugs can cure your cancer? Far from it! Ask, why do we see failures after failures being repeated over and over again? It appears that failures seems to be the norm rather than an exception.
I have one suggestion for those who want to do something! Think about it seriously.
Granted, chemo-drugs sometimes can make the tumour markers drop to normal level or the tumour shrunk completely after the treatment. But what do you do after this achievement? Send the patient home and ask him to live the same style of life that he/she had before — the earlier life that promoted his/her cancer?

- What if we have a program that teaches patients how to live a healthy life after being effectively treated?
- What if we teach them to change their life style and diet?
- What if we ask them to take supplements, vitamins or herbs to make them healthy?
- What if we ask them to take time to exercise?
These are things that patients can do for themselves when they go home after their “apparently successful” medical treatment. Above all, these are “harmless” efforts that can result in a better and healthier cancer-free life.
- In short, why can’t the medical establishment work together with the alternative healers to try and help patients prevent or minimize their cancer recurrence?
At CA Care we teach patients all the above. We take over after patients decide not to go for any more medical treatments. And often for those who are really committed, we succeeded in helping patients to heal themselves.
























You must be logged in to post a comment.